Forms (Examples and Templates), Policies, and Procedures
Volunteer Driver Program Toolkit
Section 8 – Forms (Examples and Templates), Policies, and Procedures
The forms (examples and templates), policies, and procedures included in this section are updated versions of those included in the original Washington State Volunteer Program Guidebook (2013). They are composites of similar forms, policies, and procedures used by many of the contributing programs. Many of the examples use Washington State references (and links to websites). Review the examples but use what works best for your program.
Each volunteer driver program is advised to carefully read all elements in individual forms, policies, and procedures and edit to reflect its state and local policies and practices.
The items in red should be customized for the program and its own local policies. The term "sponsoring organization" has been used uniformly so that users can easily search and replace that name with the name of their program. The items in blue are additional notes and instructions related to customizing a template. Please make sure to delete these comments in the final policy document.
The materials can be freely downloaded and edited; however, forms and policies should always be reviewed by your legal counsel to ensure compliance with state and local laws and for liability purposes. This caveat particularly applies to the policy examples, such as confidentiality.
Please Note: The FBI Records Request form is a sample. The official paper form from the FBI must be used to submit a formal records request to the FBI.
In addition to the resources included here, users are encouraged to review the examples gathered from the case studies. See Appendix to Section 7 – Case Studies.
- Abuse, Neglect, Abandonment, and Exploitation
- Bloodborne Pathogen Exposure Control Plan
- Child/Adult Abuse Record of Search Guidelines
- Code of Ethics
- Confidentiality Policy
- Disqualifying Crimes
- Donation and Contribution Request Policies
- Driver Code of Conduct
- Driver Job Description - Personally Owned Vehicle (POV)
- Driver Orientation
- Drug Free Workplace Policy
- Driver Selection Guidelines
- Driver Selection Standards
- Essential Driver Functions
- Harassment Policy
- Health/Social Services Training Content
- Liability, Standards, and Indemnification
- Meal and Incidental Expenses Reimbursement Policies
- Rider Grievance Procedure
- Training Standards
- Waivers, Agreements to Participate, and Hold Harmless
- Adult Protective Services Reporting
- Back-up Plan for Daily Operations with Sample Emergency Card
- Back-up Plan for Vehicle Loans or Out-of-Area Service
- Volunteer Driver Availability
- Driver Evaluation
- Driver Medical/Physical Release
- Driver Reference Form
- Driver Road Test
- Driver Statement of Medical Condition
- Driver Statement of Understanding
- Driver Training Checklist
- Exit Interview
- Exposure Incident Report
- FBI Fingerprint Form (Sample)
- Incident and Collision Report
- Incident Report - Volunteer Driver
- Lift Operation Procedures and Checklist
- Personnel Checklist
- Pre-Trip Inspection and Checklist
- Pre-Trip Inspection Form
- Private Vehicle Registration
- Rider Registration/Trip Request
- Transportation Request
- Trip Description
- Trip Voucher
- Volunteer Driver Job Application
- Volunteer Transportation Program Client Survey
Policies and Procedures
Adult - Abuse, Neglect, Abandonment, & Exploitation
Adult - Abuse, Neglect, Abandonment, & Exploitation
(Washington State Example)
It is important not to try to investigate on your own, but to report your concerns immediately to the office of the State Department of Social & Health Services that is responsible for Adult Protective Services. They will investigate and take action to prevent, correct, or remedy the situation, with the consent of the older person involved. The staff member (including volunteers) shall also report concerns to their supervisor to receive further instructions as needed. People in certain professions are mandated to report suspected abuse, neglect, exploitation or abandonment of persons sixty years of age or older who have a functional, mental, or physical inability to care for or protect themselves. Those mandated to report include:
- Police officers
- Social workers
- Employees* of welfare, mental health, or health agencies, or congregate care long term care facilities
- Licensed health care providers
- Employees of the Dept. of Social & Health Services
- Employees of social service agencies
*Note: Employees includes volunteers.
Persons who are required to report must call Adult Protective Services immediately, and follow up with a written report within ten (10) days.
Abuse and neglect of older persons includes several categories of acts and/or omissions generally referred to as abuse, neglect, exploitation, and abandonment. Signs of potential abuse or neglect include:
- An elderly person with bruises, welts or burns or evidence of physical restraints.
- An elderly person who appears over-or under-medicated.
- An elderly person with inadequate food or water, or with unclean clothes of bedding.
- An elderly person whose caregiver abuses alcohol or is emotionally unstable.
- An elderly person who previously has had excellent credit or resources but now seems unable to meet expenses.
- An elderly person whose caregiver is under severe stress such as illness, unemployment or family problems
- An elderly person living in a family with a history of violence such as child or spouse abuse.
- An elderly person who is not permitted visitors or direct, private communications with others.
Definitions:
Abuse: An act of physical or mental mistreatment or injury that harms or threatens a person through action or inaction by another individual. Abuse may be physical, sexual, verbal, or emotional. "Medical” abuse refers to over medication or withholding of medications or other needed assistance in order to control the older person.
Signs of abuse:
- Suspicious bruising or other injuries to arms, face, or head.
- Marks from tying or other restraints.
- Purposeful isolation.
- Unwarranted sedation.
- Withholding of food, water, or medication (without consent).
- Unexplained depression or anxiety.
Neglect: A pattern of conduct resulting in deprivation of care necessary to maintain minimum physical and mental health. Neglect occurs when; a caregiver does not provide enough care and support to meet the person's individual needs for physical emotional well-being. (The situation may be “self-neglect” when the needs of an older person are not being met, but there is not an identified caregiver.)
Signs of neglect:
- Inadequate food or water.
- Uncleanliness.
- Serious bedsores.
- Social isolation.
- Lack of proper medical or dental care or equipment.
- Unsanitary conditions.
- Unpaid bills.
- Untreated mental illness.
Exploitation: Illegal or improper use of a vulnerable adult or that adult's resources for another person’s profit or advantage. Exploitation may involve obtaining access to and misusing an older person's income, financial resources or real property, obtaining money fraudulently, charging for services riot provided, misuse of a Power of Attorney, and emotional pressure to change a will sign over property.
Signs of exploitation:
- Sudden change in an older person’s spending habits.
- Unexplained loss of resources or valuables.
- Overdrawn accounts.
- Loss checks or passbooks.
- Unusual or suspicious withdrawals from bank.
- An unfit person moving in.
- Sudden quit-claim deeds of property.
- Suspicious or unauthorized use of an older person’s credit cards.
Abandonment: Leaving a vulnerable adult without the means to obtain food, clothing, shelter, or health care. This form of abuse involves a recognized caregiver who has been giving regular and substantial care to an older person, and willfully discontinues the care without assuring adequate replacement or giving appropriate notice to responsible parties.
Signs of abandonment:
- Sudden departure of caregiver.
- No movement in or around an older person’s home.
- No answer to telephone.
- Uncollected mail or newspapers piling up.
- Older person suddenly discontinuing routine social contacts.
I have reviewed and understand __(insert name of sponsoring organization)__’s Policy regarding the reporting of abuse, neglect, exploitation, and abandonment of adults.
Signed: ___________________________________ Date: ______________________
Bloodborne Pathogen Exposure Control Plan
BLOODBORNE PATHOGEN EXPOSURE CONTROL PLAN (Example)
POLICY
The policy of __(insert name of sponsoring organization)__ is to comply with all statutory obligations and to apply all known and reasonable procedures to prevent the exposure of its employees and volunteers to potentially infectious materials.
BACKGROUND
The mission of __(insert name of sponsoring organization)__ is to provide safe, courteous, reliable transportation services to the people within our service area. In fulfilling this mission our employees and volunteers and volunteers may be exposed to body fluids, such as blood or other potentially infectious materials. While their risk of exposure is minimal, it is important for all employees and volunteers to have current information about bloodborne diseases, their methods of transmission, and preventive measures which will reduce risk of exposure. Because of their assignments, __(insert name of sponsoring organization)__’s employees and volunteers are at different levels exposure risk. Therefore, this Exposure Control Plan contains general requirements that pertain to all employees and volunteers and specific requirements that pertain only to the employees and volunteers in that department.
PURPOSE
The purpose of this Exposure Control Plan is to:
- Increase employee awareness and understanding of the bloodborne diseases, Human Immunodeficiency Virus (HIV) and Hepatitis B Virus (HBV).
- Instruct employees and volunteers concerning the transmission of HIV and HBV.
- Alleviate employee fears associated with HIV and HBV.
- Reduce employee risk of exposure to infection through the implementation of engineering and work practice controls and the provision of personal protective equipment.
RESPONSIBILITY
__(insert name of sponsoring organization)__ has the responsibility to develop a formal infection control program "tailored to the needs of the particular operation and to the type of hazards involved." This includes the following elements:
- Training about bloodborne pathogen diseases and universal precautions.
- Offering HBV vaccinations for those employees and volunteers identified as at risk.
- Providing the proper equipment.
At-risk employees and volunteers are responsible for adopting behaviors at work that prevent or reduce their risk of exposure. These behaviors include following procedures and using appropriate equipment as described under the Universal Precautions section of this plan.
CLASSIFICATION OF WORK
__(insert name of sponsoring organization)__ will provide an opportunity for all of its employees and volunteers to receive training about bloodborne pathogen diseases and precautions that can reduce their risk of exposure. However, this plan applies to those employees and volunteers who in the course of their assigned duties have a "reasonably anticipated potential for exposure to blood and/or other potentially infectious materials.” A review of all positions at __(insert name of sponsoring organization)__ identified the following job classifications as having a risk of exposure for all employees and volunteers in these classifications:
- Drivers
- Dispatchers
- Maintenance personnel
TRAINING
__(insert name of sponsoring organization)__ will train all employees and volunteers who have been identified as having an occupational risk of exposure in the provisions of this standard, the bloodborne diseases, and the universal precautions established for their particular job assignments. This training will take place within 1 month of assignment to tasks where occupational exposure may take place and at least annually thereafter.
__(insert name of sponsoring organization)__ will make training available to all employees and volunteers regarding bloodborne pathogens and universal precautions. For some job descriptions this training will be included in the established position training.
INFECTION CONTROL PROCEDURES
- Medical Abatement
__(insert name of sponsoring organization)__ will offer the Hepatitis B vaccination series without charge to all employees and volunteers in positions identified as having a risk of exposure within 1 month of their initial assignment to that position. Employees and volunteers may obtain the vaccination series through the (Name of Health District). Each affected employee must complete and sign a Hepatitis B Vaccination Decision Form. A copy of this form will be placed on file with the appropriate safety program manager and in the employee's medical record file. - Universal Precautions
Universal precautions is a system of infectious disease control that assumes that every direct contact with body fluids is infectious and requires every employee exposed to direct contact with body fluids to be protected as though the fluids were HIV or HBV infected. __(insert name of sponsoring organization)__ employees and volunteers will follow established engineering and work practice controls and use appropriate personal protective equipment to prevent contact with blood or other potentially infectious materials. Under circumstances in which differentiation between body fluids types is difficult or impossible, all body fluids shall be considered potentially infectious materials.
PATHOGEN EXPOSURE CONTROL PLAN - UNIVERSAL PRECAUTION PROCEDURES (Methods of Control)
DRIVERS
- Personal Protective Equipment
- __(insert name of sponsoring organization)__ will equip vehicles with paper towels and first aid kits which have latex or vinyl gloves, one way valve mouthpieces, tongs, sharps containers and disinfectant materials.
- Collection and Disposal Practices
- Drivers who discover syringes or other items that may be contaminated with potentially infectious material shall notify dispatch. Trained personnel, wearing gloves, will remove the item and place any needles or like items in a sharps container.
- If body fluids are spilled on a van, Drivers shall notify the manager and request instructions. Cleanup of these body fluids will be done by personnel trained in universal precaution methods.
- Laundry such a blankets, clothing, cleaning materials, etc. that is overtly contaminated with blood or body fluids, shall be double-bagged in red plastic bags, or in a bag labeled "biohazard" and treated with bleach. These bags can be thrown in secure dumpsters. If an employee's clothing and check with a supervisor regarding the treatment or disposal of the items.
- In the case of an accident involving injury(ies), if employees or volunteers choose to provide initial first aid, they should follow universal precaution procedures including wearing gloves and using a one-way valve mouth piece.
MAINTENANCE
- Personal Protective Equipment
__(insert name of sponsoring organization)__ will provide the following: utility gloves, face shields, eye protection, grabbers or tongs, sharps disposal containers, and red plastic garbage bags. - Gloves - __(insert name of sponsoring organization)__ will provide latex or vinyl gloves. Employees and volunteers will ensure gloves have no holes or discoloration prior to use and shall always have an extra pair. Gloves shall be worn when the employee has the potential for the hands to have direct skin contact with infectious waste, or while handling items or surfaces soiled with blood or other potentially infectious materials. Disposable gloves shall not be reused. Utility gloves may be washed for reuse. Any gloves will be thrown away if punctured or torn. While wearing gloves, employees and volunteers should not handle any personal items such as combs, wallets, pens and should avoid touching their faces or eyes.
- Band-Aids - Employees and volunteers will cover any open cuts, sores, abrasions, chapping, or wounds on their skin with a bandage or Band-Aids. (Particularly important for chapped hands, dermatitis).
- Face shields/eye protection - Masks, eye protection or chin-length face shields shall be worn whenever eyes, nose, or mouth might be splashed by body fluids or cleaning solution.
- Grabbers/tongs - As much as possible, employees and volunteers shall use "grabbers" or tongs and gloves to pick up potentially infectious materials. Gloves must be worn before picking up these materials and where feasible, grabbers, shovels, rakes, or other tools will be used to pick up materials (such as piles of leaves or trash) that may contain unknown objects.
- Paper towels - Used to clean up potentially infectious matter.
- Red Bags - Put all disposable (non-sharps) contaminated, or possibly contaminated, waste in red bags.
- Sharps Containers - Put all sharp objects, i.e., broken glass, needles, small sharp steel, into sharps container. DO NOT RE-CAP NEEDLES!!!
- Employees and volunteers must wear gloves while cleaning equipment which may have been exposed to potentially infectious body fluids. After cleaning equipment, employees and volunteers should discard gloves.
- Collection and Disposal Practices
- Needles - Hold discarded hypodermic needles by the barrel and place needle- down in the rigid, leak and puncture-proof sharps containers provided by the Agency. DO NOT EVER re-cap, break, bend, or dismantle a needle or syringe unit.
- Cap the sharps container when it is between one-half and three-quarters full. The container will be sealed, labeled, and stored as hazardous material. DO NOT dispose of in garbage cans or in the dumpster. Sharps containers will be disposed of by the program manager when quantities warrant.
- Condoms - May be thrown in the red bag.
- In the case of an accident involving injuries, tow truck crew members and other maintenance employees servicing the vehicle at the site will avoid contact and wear protective equipment where there is the possibility that the vehicles involved may be contaminated with body fluids. Maintenance personnel should contact a Maintenance supervisor if they suspect human debris has contaminated the vehicle(s). The Supervisor will contact County Police if needed.
- Employees and volunteers shall not use any body part such as feet, hands, etc., to compact trash.
- Feces/blood/vomit -DO NOT place human or animal feces in the trash. Disposal options are:
- Flush it down a toilet that is part of the sanitary sewer system.
- Animal feces may be buried on site.
- Human feces/blood/vomit may be washed down a drain that is part of the combined sanitary system, i.e., it winds up in the treatment plant. It is not acceptable to wash it into a storm drain as this is in direct violation of State and Federal codes.
- Laundry such as blankets, clothing, cleaning materials, etc. that is overtly contaminated with blood or body fluids, shall be double-bagged in red plastic bags, or in a bag labeled "biohazard" and treated with bleach. These bags can be thrown in secure dumpsters. If an employee's clothing becomes contaminated, the employee shall change out of the contaminated clothing and check with a supervisor regarding the treatment or disposal of the items.
- Personal Protection Procedures
- Gloves worn during contact with potentially infectious body fluids shall be removed in the following manner:
- With the right hand, pinch the palm of the left glove and pull left glove down and off your fingers. Form left glove into a ball and hold it in the fist of your right hand.
- Insert two fingers of left hand under the inside rim of your right glove on the palm side.
- Push glove inside out down onto your fingers and over balled left glove.
- Grasp gloves, which are inside out and together - with your left hand and remove them from your right hand
- Discard gloves.
- After removing gloves WASH HANDS!!! Employees and volunteers shall wash their hands with soap and water immediately or as soon as possible after working with blood or other potentially infectious materials. Proper hand washing requires the use of soap and vigorous scrubbing for approximately 5 seconds, followed by 5 seconds of rinsing. Remember fingernails when washing hands.
- Employees and volunteers will follow normal hygiene practices, including washing of their hands at regular intervals throughout the day and especially before eating, drinking, smoking, applying cosmetics or lip balm, handling contact lenses, or putting anything in the mouth during the day, if they have been working in an area where there is potential for occupational exposure. Commercially packaged moistened towelettes are an acceptable alternative when soap and water are not available.
- If eyes are exposed, flush for 5 minutes with clean water.
POST-EXPOSURE PROCEDURES
- Any employee who experiences a needle stick; splash of blood or body fluids to the eyes, nose, mouth, open wounds, or to chapped, abraded, or otherwise damaged skin; or human bite with broken skin shall:
- Wash the affected area as quickly as possible with soap and water or cleaners to reduce contamination; or flush with water if the eye is affected.
- Immediately notify their supervisor. Both will treat the exposure as an industrial injury and will follow those procedures.
- The incident report for bloodborne pathogen exposure will contain the following elements:
- Documentation of the route(s) of exposure, and circumstances under which exposure incident occurred;
- The employee will then follow these procedures:
- Seek medical attention, no later than 24 hours after exposure.
- Follow the physician's recommendations regarding possible Hepatitis B vaccination, Hepatitis B Immune Globulin (HBIG) injection, and follow-up treatment.
- Report and week medical care for any acute illness that occurs within 12 weeks after the exposure, especially one characterized by fever, rash, or disease of the lymph nodes.
- The physician shall collect blood from the exposed employee as soon as possible after the exposure incident for the determination of HBV/HIV status. Actual testing may be done at that time or a later date if the employee so requests. Results are confidential, and are released only to the person tested. Confidentiality of the results are waived if the employee files a subsequent insurance disability claim.
- An employee who tests negative for HBV/HIV should be retested at 6 weeks, 12 weeks, and 6 months after exposure to determine whether transmission has occurred.
- If the employee or volunteer refuses to submit to #1 and 2 above, they will be required to complete a Hepatitis B Vaccination decision form indicating the decision to decline the vaccinations.
- The appropriate manager must be notified when an exposure occurs.
IMMUNIZATIONS
__(insert name of sponsoring organization)__ will offer the Hepatitis B vaccination series to all employees and volunteers who have been identified as having risk of exposure. All employees and volunteers in these positions must complete a "Hepatitis B Vaccination Decision Form" that will be kept in the employees and volunteers' medical records files. In addition, a copy will be kept on file with the appropriate safety personnel.
RECORDKEEPING
__(insert name of sponsoring organization)__ will establish and maintain an accurate record of each occupational incident. As required by the OSHA standard, this record will include:
- The name and social security number of the employee.
- A copy of the employee's HBV vaccinations and any medical records relative to the employee’s or volunteer’s ability to receive vaccination.
- A copy of all results of examinations, medical testing, and follow-up procedures.
- The employer's copy of the healthcare professional's written opinion. A copy of the information provided to the healthcare professional.
__(insert name of sponsoring organization)__ ensures that such records will be kept confidential and will not be disclosed or reported without the employee's or volunteer’s express written consent to any person within or outside the workplace except as required by the standard, or law.
__(insert name of sponsoring organization)__ also will maintain a record of all training related to this standard. This record will include:
- The dates of the training sessions.
- The contents or a summary of the training sessions.
- The names and qualifications of persons conducting the training.
- The names and job titles of all persons attending the training sessions.
GLOSSARY
- Bloodborne Pathogens - pathogenic microorganisms that are present in human blood and can cause disease in humans; include, but are not limited to, hepatitis B virus (HBV) and human immunodeficiency virus (HIV).
- Collateral exposure risk - potential skin, eye, mucous membrane, or parenteral contact with blood or other potentially infectious materials that may result from situations in which they are placed because of their positions within the organization.
- Exposure Incident -a specific eye, mouth, other mucous membrane, or parenteral contact with blood or other potentially infectious materials that may result from situations in which they are placed because of their positions within the organization.
- Occupational Exposure - reasonably anticipated skin, eye, mucous membrane, or parenteral contact with blood or other potentially infectious materials that may result from the performance of an employee's duties.
- Other Potentially Infectious Materials - Include:
- Human body fluids: semen, vaginal secretions, cerebrospinal fluid, synovial fluid, pericardial fluid, peritoneal fluid, amniotic fluid, any body fluid visibly contaminated with blood, and all body fluids in situations where it is difficult or impossible to differentiate between body fluids;
- Any unfixed tissue or organ (other than intact skin) from a human (living or dead).
- Sharps - any object that can penetrate the skin including, but not limited to, needles, broken glass, and wires.
SUMMARY
This Exposure Control Plan contains the framework through which __(insert name of sponsoring organization)__ addresses bloodborne pathogen safety issues. Procedures specific to each Department are contained within their safety and training documents and materials. This plan will be reviewed and updated annually or whenever new tasks and procedures affect occupational exposure. It will be made accessible to employees and volunteers.
Child/Adult Abuse Record Search Guidelines
Child/Adult Abuse Record Search Guidelines
(Washington State Example)
Refer to Revised Code of Washington (RCW) [43.43.830-43.43.845] for complete and current information. Child/Adult Abuse Background checks may be conducted only by Washington State business, organizations or individuals, all other states must conduct searches under the Criminal Records Privacy Act.
- Searches can be conducted only on prospective employees, volunteers or adoptive parents. (For current employees or volunteers, see note below.)
Background checks can be requested on prospective employees, volunteers or adoptive parents who will or may have unsupervised access to children under sixteen years of age, developmentally disabled persons, or vulnerable adults. The background check is for initial employment or engagement decisions only. - Applicants must be notified an inquiry may be made.
A business or organization shall not make an inquiry to the [Washington State Patrol] unless the business or organization has notified the applicant, who has been offered a position as an employee or volunteer, an inquiry may be made. - A signed disclosure statement is required from applicant before a search is conducted.
A business or organization shall require each applicant to disclose to the business or organization whether the applicant has been: - convicted of any crime against children or other persons;
- convicted of crimes relating to financial exploitation if the victim was a vulnerable adult;
- convicted of crimes related to drugs as defined in [RCW 43.43.830];
- found in any dependency action under [RCW 13.34.040] to have sexually assaulted or exploited any minor or to have physically abused any minor;
- found by a court in a domestic relations proceeding under [Title 26 RCW] to have sexually abused or exploited any minor or to have physically abused any minor;
- found in any disciplinary board final decision to have sexually or physically abused or exploited any minor or developmentally disabled person or to have abused or financially exploited any vulnerable adult;
- found by a court in a protection proceeding under chapter [RCW 74.34], to have abused or financially exploited a vulnerable adult.
The disclosure shall be made in writing, signed by the applicant, and sworn under penalty of perjury. The disclosure sheet shall specify all crimes against children or other persons, all crimes relating to drugs, and all crimes relating to financial exploitation as defined in [RCW 43.43.830] in which the victim was a vulnerable adult.
- Applicants must be notified of the response.
The requesting agency shall notify the applicant of the state patrol’s response within ten days after receipt. The employer shall provide a copy of the response to the applicant and shall notify the applicant of such availability.
Notes:
- The business or organization shall use this record only in making the initial employment or engagement decision. Further dissemination or use of the record is prohibited. A business or organization violating this subsection is subject to a civil action for damages.
- Background checks pursuant to the Child and Adult Abuse Information Act do not expire and therefore should not be conducted routinely.
- Background checks on current employees or volunteers should be done through the Criminal Records Privacy Act, [RCW 10.97].
- Responses are limited to [Washington State records] only.
Code of Ethics
Code of Ethics (Washington State Example)
This code of ethics governs the performance of __(insert name of sponsoring organization)__’s officers, employees, board members, volunteers, and agents, (representatives) engaged in the administration of contracts supported by Federal assistance. Any employee in violation of these policies is subject to disciplinary action as outlined in the Employee Handbook. Any officer or board member who violates these policies will be subject to disciplinary action as determined by a majority vote of the Board of Directors. Any volunteer who violates these policies will be subject to disciplinary action as determined by the manager of the program in which the person volunteers.
- Gifts: Representatives shall not accept gratuities, favors, gifts, or anything of monetary value (over $5.00) from present or potential contractors or sub-recipients.
- Personal Conflict of Interest: Representatives who participate in the selection, award, or administration of a contract supported by Federal funds are prohibited from a real or apparent conflict of interest. Such a conflict would arise when any of the parties below has a financial or other interest in the entity selected:
- a __(insert name of sponsoring organization)__ representative;
- any member of the representative’s immediate family;
- the representative’s partner;
- an organization that employs, or is about to employ, any of the above.
- Organizational Conflict of Interest: __(insert name of sponsoring organization)__ is prohibited from real or apparent organizational conflicts of interest. Such a conflict when the nature of the work to be performed under a proposed third party contract may, without some restrictions on future activities, result in an unfair competitive advantage to the third party contractor or impair its objectivity in performing the contract.
- Bonus or Commission: __(insert name of sponsoring organization)__ affirms that it has not paid, and agrees not to pay, any bonus or commission for the purpose of obtaining approval of its application for Federal financial assistance
- Restrictions on Lobbying: __(insert name of sponsoring organization)__ agrees to comply with the provisions of 31 USC 1352, which prohibits the use of Federal funds for lobbying any official or employee of any Federal agency, or member or employee of Congress. In addition, even though no Federal funds are use, __(insert name of sponsoring organization)__ agrees to disclose any lobbying of any of any official or employee of any Federal agency, or member or employee of Congress in connection with Federal assistance and to comply with USDOT regulations “New Restriction on Lobbying,” 49 CFR Part 20.
- Employee Political Activity: The terms of the “Hatch Act,” 5 USC Section 1501 through 1508, and office of Personnel Management regulations, “Political Activity of State or Local Officers or Employees,” 5 CFR Part 151, apply to supervisory employees of __(insert name of sponsoring organization)__.
- False or Fraudulent Statements or Claims: __(insert name of sponsoring organization)__ acknowledges that it will not make a false, fictitious, or fraudulent claim, statement, submission or certification in conjunction with any program supported by Federal assistance. __(insert name of sponsoring organization)__ is aware that Federal penalties could be imposed for making a false, fictitious, or fraudulent claim, statement, submission or certification in conjunction with any program supported by Federal assistance.
My signature below acknowledges understanding of __(insert name of sponsoring organization)__’s Code of Ethics:
Signature: __________________________________________ Date: ___________
Confidentiality Policy
Confidentiality Policy (Washington State Example)
The principal of confidentiality is basic to the maintenance of professional ethics and community respect. All staff and volunteers of __(insert name of sponsoring organization)__ have a set of ethical responsibilities by which they are bound to the rider, the community, and themselves. __(insert name of sponsoring organization)__ riders act in good faith, expecting their circumstances and personal matters to remain confidential and __(insert name of sponsoring organization)__ is obligated by law and ethics to reciprocate. Confidentiality of rider information is maintained for the protection of the rider and for __(insert name of sponsoring organization)__.
Staff members, including volunteers, will use the following procedures. For the purposes of these procedures a "rider" is defined as a person registered as a program participant. Registration is accomplished by completion of a Rider Information Form (RIF).
- All staff members will take responsibility for protecting the confidentiality of all riders. New staff members will receive instruction in these confidentiality procedures.
- All written and unwritten information concerning riders of __(insert name of sponsoring organization)__ are considered as confidential.
- All written information regarding the riders of __(insert name of sponsoring organization)__ will be maintained in files. Only those staff members with a "need to know" will have access to these files. No staff member may remove rider files from the office without authorization from the staff member's supervisor.
- When it is necessary for a member of the staff to communicate information about a rider to another person or agency, a Release of Information Form will be signed by the rider or their legal representative. The signed release will be kept in the rider's permanent record. If the rider is unable to give written consent then the staff member releasing the information will document the circumstances.
- When rider-related materials, i.e., lists, log and files are used outside the office, staff members are responsible and must take appropriate steps to safeguard the materials.
- In emergency situations, when it is not possible to have a form signed, a verbal release may be given by the rider or their legal representative. The staff member who receives the verbal release will make a note in the rider's file and will obtain the written release as soon as possible.
- A signed release may not be needed when the information is used for specific purposes. [DSHS Notice of Privacy Practices for Client Medical Information (November 1, 2024)]
- When a __(insert name of sponsoring organization)__ staff member is working with a rider and finds it necessary to obtain written information from another person or agency, it will be necessary to obtain a signed release from the rider or representative. This release will indicate that the rider or representative has given permission for release of information to __(insert name of sponsoring organization)__.
- When a __(insert name of sponsoring organization)__ staff member either receives requested written information or releases written information about a rider to another person or agency, a written or verbal follow-up will be given to the rider. This follow-up will inform the rider as to what information was released or obtained and what progress has been made in helping with their individual situation. A record of the follow-up will be kept in the rider's file.
- When a staff member receives unsolicited information from the rider the staff member may legally need to share that information, e.g., suspected abuse. The staff member may also ask the rider for permission to make an appropriate referral, i.e., [Gatekeeper] function.
- When a staff member receives unsolicited information about a rider from family members, [Gatekeepers], etc. the staff member may share in the information with the rider. Professional judgment will determine what to share.
- The fact that a situation has been made public through any of the new media does not alter the fact that this person still has confidentiality privileges with __(insert name of sponsoring organization)__. For example, if a rider has been having difficulties with a given problem and is arrested, __(insert name of sponsoring organization)__ confidentiality procedures will be maintained.
- The fact that a case has been made public through any of the news media does not alter the fact that this person still has confidentiality privileges with __(insert name of sponsoring organization)__. For example, if a client has been having difficulties with a given problem and is arrested, __(insert name of sponsoring organization)__ confidentiality procedures will be maintained.
I have read and understand the above Confidentiality Policy:
Signature: __________________________________________ Date:___________
Disqualifying Crimes (Washington State Example)
Disqualifying crimes are addressed in three areas by [Washington Administrative Code (WAC)]. Regulations of executive branch agencies are issued by authority of statutes. The [WAC] codifies the regulations and arranges them by subject or agency. The online version of the [WAC] is updated twice a month and should always be referenced for the most current regulations. Copies of the [WAC] as they existed each year since 2004 are available in the [WAC archive].
Permanent Prohibitions – Criminal convictions permanently prohibiting licensing, contracting, or authorizing unsupervised access to children or to individuals with developmental disability. [WAC 388-06-0170]
Other Prohibitions –Other criminal convictions that prohibit working with children or individuals with a developmental disability. Disqualification if it has been less than five years from time of conviction. [WAC 388-06-0180]
Exceptions –Persons with convictions may be able to have unsupervised access to children or individuals with a developmental disability under limited circumstances. [WAC 388-06-0190]
Donation and Contribution Request Policies
Donation Policy(Washington State Example)
- Riders of volunteer transportation networks should be those persons, including their personal attendants, who because of physical or mental disability, income status, or age (too old or too young) are unable to transport themselves or purchase appropriate transportation.
- Persons who receive services funded by Title III of the Older Americans Act must be given a free and voluntary opportunity to contribute to the cost of services provided. The same opportunity must be extended to persons who receive [Senior Citizens Services Act (SCSA)], funded services that are not subject to a means test. [Chapter 74.38 Revised Code of Washington (RCW)].
- Other persons in need of special transportation, regardless of funding source, should be afforded similar opportunities, as are the persons in the categories above.
- The service provider must protect each person’s privacy with respect to his or her contribution, establish procedures to safeguard and account for all contributions made by users of the service and use all such contributions to expand the service that received the contribution.
- The service provider may develop a suggested contribution schedule. If a schedule is developed, the provider must consider the income ranges of older persons in the community and the provider’s other sources of income. No otherwise eligible person may be denied service because they will not or cannot contribute to the cost of service.
Contribution Request (Washington State Example)
- Volunteer drivers are not allowed to receive donations. In order to assure that riders are afforded the opportunities described above, the may be mailed a detailed accounting of volunteer trips provided, length of the trip, and a suggested donation rate. Those factors may be totaled in the form of an aggregate suggested donation.
- A copy of the aggregate accounting can be sent to persons who have agreed to pay for the transportation services. Included are family members, personal representatives, friends, and agencies such as [Washington Department of Veterans Affairs (DVA)] that have agreed to pay at the suggested donation rate.
Driver Code of Conduct
Driver Code of Conduct (Example)
- All volunteer drivers will act in a professional manner at all times.
- Reports of staff or volunteer driver misconduct will be the cause for immediate suspension from client service. Confirmation of misconduct shall be cause for removal of the staff or volunteer driver involved from serving clients. The manager may be required to report all incidents to the state or federal funding agencies.
- If the state funding agency(ies), and/or __(insert name of sponsoring organization)__ receives complaints regarding any volunteer driver transporting riders, and/or it is determined that the volunteer driver is not performing the service in a safe, reliable, or responsible manner and corrective action has not resulted in improved performance, the manager will remove the volunteer driver from service to riders.
- If any volunteer is suspended from service due to complaints or a determination that the person is not performing the service in a safe, reliable, and responsible manner they will not return to service until the manager has developed a Plan of Improvement.
- Volunteers shall perform the following minimum levels of service:
- A volunteer driver shall not:
- Make sexually explicit comments, or solicit sexual favors, or engage in sexual activity;
- Solicit or accept controlled substances, alcohol, or medications from riders;
- Solicit or accept money from riders;
- Use alcohol, narcotics, or controlled substances, or be under their influence, while on duty. Prescribed medication can be used by a driver as long as their duties can still be performed in a safe manner and __(insert name of sponsoring organization)__ has written documentation that medication will not impact the ability of the driver;
- Eat or consume any beverage while operating the vehicle or while involved in rider assistance;
- Smoke in the vehicle when riders are present. This rule also applies to clients and a client’s escort;
- Wear any type of headphones while on duty;
- Be responsible for passenger's personal items.
- A volunteer driver shall:
- wear, or have visible, easy to read proper organizational identification;
- as appropriate to the needs of the rider, exit the vehicle to open and close vehicle doors when passengers enter or exit the vehicle and provide assistance as necessary to or from the main door of the place of destination;
- properly identify and announce their presence at the entrance of the building at the specified pick-up location if a curbside pick-up is not apparent, or with attending facility staff;
- assist the passengers in the process of being seated, including the fastening of the seat belt, when necessitated by the rider’s condition;
- confirm, prior to allowing any vehicle to proceed, that all passengers are properly secured in their seat belts, car seats, and, when applicable, that wheelchairs and passengers who use wheelchairs are properly secured (Exception: Only a passenger who has a letter, carried on his/her person and signed by the passenger’s physician, stating that the passenger ’s medical condition prevents the rider from using a seat belt, may be transported without a fastened seat belt);
- provide an appropriate level of assistance to passengers, when requested, or when necessitated by a passenger’s condition;
- provide support and direction to passengers. Such assistance shall also apply to the movement of wheelchairs and mobility-limited persons as they enter or exit the vehicle using the wheelchair lift/ramp, as applicable. Such assistance shall also include stowage by the driver of mobility aids and folding wheelchairs;
- be clean and maintain a neat appearance at all times;
- be polite and courteous to riders; riders shall be treated with respect and in a culturally appropriate manner when receiving transportation services. The manager should notify the volunteer driver of any known cultural issues significant to providing transportation services.); and,
- respect passenger’s rights to confidentiality.
I have received a copy of the above Driver Code of Conduct and will abide by the contents:
Signature: ________________________________________ Date: ________________
Driver Job Description – Personally Owned Vehicle (POV)
Volunteer Transportation Driver (POV) (Example)
POSITION TITLE: Volunteer Driver
PURPOSE OF JOB: To provide transportation requested to families or individuals to help them access necessary services.
DUTIES OF POSITION: To be a careful and responsible driver.
To meet requests promptly as assigned.
To call immediately if unable to keep an assigned request.
To report any problem stemming from a transportation assignment immediately.
JOB QUALIFICATIONS: Must have a valid driver’s license and good driving record (Records will be checked).
Must have vehicle liability insurance policy at least at State minimums. Must maintain vehicle in good working condition.
Must have access to a phone.
Must have and use seat belts. Must require use of car seats for infants and toddlers. Car seats will be provided by the (sponsor organization).
Willing to have children and small adults ride in the back seat if passenger side airbags are present and activated.
For the purpose of state insurance, volunteer status begins at the time the volunteer leaves their home or other point of dispatch.
REQUIRED COMMITMENTS: Must enjoy being with people and have desire to help with transportation of individuals with needs for special transportation.
Must follow volunteer Statement of Understanding.
JOB BENEFITS: Satisfaction of working with persons in need.
Reimbursement for mileage at the state’s current rate and other out-of-pocket expenses.
Auto liability coverage over and above the policy amount carried by the Volunteer.
Personal liability insurance at $1,000,000.
Medical insurance though the State’s Workman’s Compensation program.
Errors and Omissions insurance at $1,500,000.
Driver Orientation
Driver Orientation (Example)
The __(insert name of sponsoring organization)__ is required to provide orientation to volunteers prior to their providing service. Orientation shall include:
- Information about __(insert name of sponsoring organization)__.
- The purpose of the Volunteer Transportation Program.
- The role volunteers play in providing services.
- An explanation and a copy of the job description.
- A statement that the volunteer’s personal auto insurance is their primary coverage, and
- That the volunteer should review their policies to ensure that there is not language that would prohibit the volunteer from providing volunteer transportation.
- That the Volunteer Agency maintains coverage only in excess of the driver’s personal coverage.
- Explains what additional coverage __(insert name of sponsoring organization)__ maintains covering volunteers.
- Volunteer’s Rights and Responsibilities. Minimum requirements include:
- To maintain their vehicle in safe operating condition
- To assure that the vehicle has operable seat belts and that all passengers and the volunteer driver shall use them.
- To maintain client confidentiality.
- To exercise due care in operating the motor vehicle.
- Reimbursement for mileage and other direct travel expenses.
- Reporting requirements.
- Evaluation.
- __(insert name of sponsoring organization)__ contact and supervision.
- Accident and other incident reporting.
Driver Selection Guidelines
Volunteer Driver Selection Guidelines (Washington State Example)
A good driver is the most important ingredient in any volunteer program. __(insert name of sponsoring organization)__ has established specific driver guidelines to qualify those persons who have volunteered to drive a public vanpool vehicle and to assure safe, reliable transportation to the public. Because the responsibilities of a volunteer driver include defensive driving and getting a group of people to and from work on time, a number of important items must be reviewed.
- A record (abstract) of the applicant's personal and employment driving history will be obtained.
- A [Washington] State Criminal History Background Check will be obtained by __(insert name of sponsoring organization)__.
- An FBI Fingerprint Criminal History Background Check.
Selection of volunteer drivers is primarily dependent upon the following:
LICENSE AND EXPERIENCE: A potential volunteer driver must possess a valid [Washington] State Driver's License and have driven for at least 5 years.
AGE: A potential volunteer driver must be at least 21 years of age.
SUSPENSION OR REVOCATION OF LICENSE: Report of a suspension/revocation within the past 5 years may cause a potential volunteer driver's application to be rejected. Report of a suspension/revocation within the last 10 years for reckless driving, hit-and-run, leaving the scene of an accident, driving while under the influence of alcohol or drugs, driving while impaired, or a felony will result in application rejection.
VIOLATIONS: Any moving violations received by a potential volunteer driver will be reviewed and may result in application rejection. A "Failure to Appear" on a driving record may result in application rejection.
ACCIDENTS: Any accident in which a potential volunteer driver has been involved will be reviewed and may result in application rejection.
INSURANCE HISTORY: Cancellation or non-renewal of insurance coverage within the past 5 years will be reviewed. If the action is related to the applicant's driving behavior, the application may be rejected. Filing of a Certificate of Financial Responsibility by a potential volunteer driver due to their personal driving record may also result in application rejection.
ABILITY TO PERFORM DRIVING FUNCTIONS: A potential volunteer driver must be able to perform essential driving functions as listed in these guidelines.
DRIVER ORIENTATION COURSE: All potential volunteer drivers must complete Driver Orientation Course before receiving final approval and before driving in the program.
Final approval for a volunteer to drive a vehicle is dependent upon successful completion of the application process, successful completion of the driver orientation course, and a personal interview with the manager. On-the- road observation of any applicant or currently approved volunteer driver may occur at any time and for any reason. Failure to meet any criteria may result in application rejection or suspension of driving privileges.
[Washington] State Legislature law allows licensed drivers aged 55 and over to receive reductions in automobile insurance premiums if they complete an approved eight hour vehicle accident prevention course. Each course includes information about the effects of aging on driving; driver problem areas such as yielding the right of way, driver awareness, speeding, passing, road signs and signals; and driving while under the influence of alcohol or drugs.
Driver Selection Standards
| Points | Citation |
|---|---|
| 1 | Defective or problem equipment |
| 1 | Not at fault accident |
| 1 | No insurance in vehicle; expired insurance |
| 1 | Improper child restraint |
| 1 | Headphones or illegal TV |
| 1 | Expired license; license not on person |
| 2 | Failure to signal |
| 2 | Illegal turns |
| 2 | Failure to yield or stop |
| 2 | Speeding (5 to 9 over) |
| 2 | Violation of school bus sign |
| 2 | Impeding traffic (traveling too slowly) |
| 2 | Following too closely |
| 2 | Illegal lane change; improper lane travel |
| 3 | Illegal passing |
| 3 | No insurance |
| 3 | Speeding (10 to 14 over) |
| 3 | Failure to appear |
| 3 | At fault accident |
| 3 | No valid license |
| 4 | Speeding (15 or over) |
| 5* | Driving with license suspended or revoked |
| 5* | Hit & run (misdemeanor) |
| 5** | Eluding a police vehicle |
| 5** | DWI, DUI, Reckless (negligent driving) |
| 5** | Vehicular assault/homicide, hit & run (felony) |
| 5** | More than one accident in 3-5 years |
| 5 | Unsatisfied bench warrant |
| * Disqualified if in last five (5) years. | |
| ** Disqualified if in last ten (10) years. |
Selection Standards(Washington State Example)
This Selection Standards list is intended as a guideline in selecting new volunteer drivers and for evaluating the ongoing records of registered drivers. A periodic check of each driver’s license record will be done at least annually. All drivers are informed of these standards for acceptable drivers and their responsibility to immediately report any citations or accidents, whether in their private auto or in a program vehicle. A potential volunteer driver is not approved until __(insert name of sponsoring organization)__’s requirements (application, motor vehicle records approval, review of selection guidelines, orientation, and a personal interview) have been satisfied.
To enable an objective evaluation of each applicant’s record, a point system has been adopted. Above the recommended point level, a person is not allowed to drive as a volunteer driver without specific approval from the manager. The system works by running the [Washington] Department of Licensing record for the applicable driver and comparing any citations or accidents that have occurred within the last three (3) years with the list of point values. The driver’s five-year record may also be reviewed in determining potential risk.
The total points are compared with the acceptable standard of four (4) or fewer points. Each citation is counted separately, even if the driver received more than one citation for the same incident. The potential volunteer driver must also meet all other standard requirements.
Drug Free Workplace Policy
Drug Free Workplace Policy (Example)
- __(insert name of sponsoring organization)__’s employees and volunteers are prohibited from the unlawful manufacture, distribution, dispensing, possession, or use of a controlled substance at any of __(insert name of sponsoring organization)__’s facilities and/or during any of the programs offered by __(insert name of sponsoring organization)__.
- Any violation of the prohibitions in item “1” above will be considered to be “Just Cause” for suspension and/or discharge under the procedures of __(insert name of sponsoring organization)__.
- As a condition of employment or registration as a volunteer each employee or volunteer will:
- abide by the terms of item “1” above and;
- notify __(insert name of sponsoring organization)__ in writing of any criminal drug status conviction for a violation occurring in the workplace no later than five calendar days after such conviction.
- __(insert name of sponsoring organization)__ will notify grantor agencies in writing within ten calendar days after receiving notice under item “3B” as referred to above, with respect to any employee or volunteer who is so convicted and will:
- Take appropriate personnel action against such an employee, up to any including termination; or
- Require such an employee to participate satisfactorily in drug abuse assistance or rehabilitation program approved for such purposes by Federal, State, or local health, law enforcement or other appropriate agency.
- The employee and/or volunteer acknowledges by signature below that they have:
- been given a copy of this policy statement;
- reviewed this policy statement, and;
- understood the policy statement.
A copy of the policy will be maintained in the volunteer’s Personnel File.
I have read and understand the above Policy.
Signature:___________________________________ Date: ____________________
Adopted by
__(insert name of sponsoring organization)__ on this date: ____________
Essential Driver Functions
Volunteer Van Driver Essential Functions (Washington State Example)
A potential volunteer driver must be able to perform essential driving functions as listed below:
- Safely operate 8-passenger, 12-passenger and 15-passenger vehicles on while adhering to an established time schedule.
- Understand, adhere to, and apply [Washington State] traffic regulations and sponsoring organization’s policies and procedures.
- Able to fuel vehicle or obtain assistance from riders or service station attendant.
- Able to clean interior and exterior of vehicle or obtain assistance from riders.
- Able to change a flat tire or obtain assistance from riders.
- Able to perform the daily inspection.
- Check for fluid leaks. Call the manager if leaks are observed.
- Check for body damage and report to the manager.
- Ensure that no obstacles are in the path of the vehicle.
- Check gauges after thirty-second vehicle warm-up. Report any irregularities to the manager.
- Ensure mirrors are clean and properly adjusted.
- Ensure windows are clean and clear of fog, ice, or snow before operating vehicle.
- Report any chips or cracks at service time or immediately if they are serious.
- Ensure that seat belts are all operational.
- Ensure that the interior of the van is clean and free of debris and that the area under the driver‘s seat is free of any items (flashlight, camera, etc.).
- Check that the brakes are working properly. Report any abnormalities immediately.
- Ensure that the steering operates properly. Report any abnormalities immediately.
- Check the exhaust system to ensure proper operation and ventilation.
- Able to perform weekly inspection. (Optional depending on program format)
- Check oil level. Add oil, using container in van, if needed (keep containers).
- Check to ensure the coolant/antifreeze level is adequate. Add fluid if needed.
- Check the windshield fluid level. Add fluid if needed.
- Check the power steering fluid level. Add fluid if needed.
- Check the transmission fluid level. Add fluid if needed.
- Check the brake fluid level. Add fluid if needed.
- Check the tire pressure and tire tread. Fill air to appropriate level.
- Report unusual tire wear.
- Check the wipers. Replace or report at next maintenance.
- Able to perform monthly inspection. (Optional depending on program format)
- Check belts and hoses. Report any unusual wear.
- Check that headlights, taillights, directional signals, and emergency flashers work properly.
- Check that the battery cable is tightly attached and free of corrosion.
- Ensure that the heater, defroster, and air conditioner work properly.
Harassment
Policy on Harassment (Example)
It is the policy of the __(insert name of sponsoring organization)__ that it will not tolerate verbal or physical conduct by any employee or volunteer which harasses, disrupts, or interferes with another’s work performance or which creates an intimidating, offensive, or hostile environment.
- All forms of harassment are prohibited but it is the __(insert name of sponsoring organization)__’s policy to emphasize that sexual harassment is specifically prohibited. Each supervisor has a responsibility to maintain the workplace free of any form of sexual harassment. No supervisor is to threaten or insinuate, either explicitly or implicitly, that an employee’s refusal to submit to sexual advances will adversely affect the employee’s employment, evaluation, wages, advancement, assigned duties, shifts, or any other condition of employment or career development. In addition, no supervisor is to favor in any way any applicant or employee because that person has performed or shown willingness to perform sexual favors for the supervisor.
- Other sexually harassing conduct in the workplace, whether committed by supervisory or non-supervisory personnel, is also prohibited. Such conduct includes:
- sexual flirtations, touching, advances, or propositions;
- verbal abuse of a sexual nature;
- graphic or suggestive comments about an individual’s dress or body;
- sexually degrading words to describe an individual; and
- the display in the workplace of sexually suggestive objects or pictures, including nude photographs or illustrations.
- Any employee who believes that the actions or works of a supervisor or fellow employee constitute unwelcome harassment has a responsibility to:
- tell the supervisor or fellow employee that their action or words are unwelcome and are considered harassment;
- report or complain as soon as possible to the appropriate supervisor or to the President of the Board of Directors if the complaint involves the director.
- All complaints of harassment must be investigated promptly in a manner that is as impartial and confidential as possible. If the employee is not satisfied with the handling of a complaint or the action taken by the manager then the Grievance Procedure should be followed.
I have read and understand the above policy and signing below constitutes an agreement to adhere to this policy.
Signature: _________________________________________Date:___________
Health/Social Services Training Content
“Gatekeeper” Training Content (Washington State Example)
The [Local Social Service Organization] is committed to enhancing lives and supporting communities with Transportation, Nutrition, Information & Assistance/Care Management, Respite, and Home Care Services. The primary mission of this community-based [Social Service Organization] is to serve older persons in their homes for as long as possible. To target and identify those older adults who may be isolated and at-risk, the [Information & Assistance/Care Management Program] depends on community members, called [Gatekeepers], to assist the staff in locating vulnerable adults who may be in need of assistance.
The [Information & Assistance/Care Management staff members] make home visits to inform older people of the services available in [Program Area]. The [Care Managers] will assess each individual's needs or concerns.
These professional staff members assist older adults with filling out forms for Social Security benefits, Medicaid, Food Stamps, in-home services Energy Assistance, and Weatherization. They help provide access to transportation services through referrals to [Local Transportation Providers]. Many older adults and persons with disabilities need part-time help in order to remain in their own homes. The [In-Home Worker Registry] provides a list of screened and qualified people who want to do yard work, housework, or serve as live-in companions. The [Care Managers] help the client interview prospective workers and suggest terms of employment.
The [Care Managers] can also help locate health appliances, such as wheelchairs, walkers, and emergency response devices, e.g., Lifeguard/Lifeline, to help the individual remain at home. The [Care Managers] help clients sort through the confusing maze of Medicare claims and insurance policies. They also introduce older adults to the [Senior Nutrition Program]; a nutritious noon meal served in a social setting in [Names of Locations]. The workers also refer people to appropriate services including Home Health, State-funded home care programs, legal services, and hearing clinics.
In order to effectively assist area older persons, help is needed from community members. As volunteer drivers you can assist by letting us know about an older person who may want to utilize our services. While we would like to know every person over 60 years of age living in the county, certain situations demand immediate attention. Those situations we feel indicate a prompt call to our office which is listed on the next page.
CALL (LOCAL SENIOR SERVICES AGENCY) WHEN YOU OBSERVE:
- Change in appearance: hair uncombed, dirty; soiled clothes; clothing inappropriate for weather.
- Condition of the home:
- Exterior/interior in need of repair
- Little or no food
- Old newspapers/possessions lying around
- Calendar on wrong month or year
- Strong odors
- Neglected pets
- Stove burner left on
- Little or no understanding of what is being said; confused; inappropriate response; not oriented to person, place, time; forgetful; repetitive; constant reminiscing.
- Depression:
- Recent loss or death of a relative, friend, or pet
- Remarks such as "I don't care...what's the use.”
- Complaints about not eating/sleeping
- Anxious, uncomfortable, fidgety appearance
- Anger; hostility directed at self, you, or another; suspicious
- Relies on tranquilizers/alcohol
- Recent personality changes
- Physical losses:
- Loss of hearing, sight
- Inability to move easily
- Chronic (continual) illness
- Numerous medicine bottles/prescriptions
- No contact with a doctor in years
- Any other changes in health
- Lack of social relationships; no mention of family or friends.
- Change in the usual support system; loss of dependable helper such as a friend or neighbor.
- Very low income or inability to manage money.
- Any person living alone over the age of 80.
PLEASE CONTACT
__(insert name of sponsoring organization)__
TO GET HELP FOR AN OLDER PERSON
PHONE: ___________________________ E-MAIL: ____________________________
Liability, Standards, and Indemnification
Liability, Standards, and Indemnification (Washington State Example)
- Liability:
- Under [RCW (Revived Code of Washington) 24.06.035], a member of a non-profit board of directors or an officer has immunity from liability as granted in [RCW 4.24.264].
- Under [RCW 4.24.264] member of a board or an officer is not individually liable for any discretionary decision or failure to make a discretionary decision within his or her official capacity as a director or officer unless the decision or failure to decide constitutes gross negligence.
- Standards:
- Under [RCW 23B.08.300] and [RCW 23B.08.420] the general standards for a director or officer are to:
- act in good faith;
- with the care an ordinary prudent person in a like position would exercise under similar circumstances; and
- in a manner the director reasonably believes to be in the best interests of the corporation.
- A director is entitled to rely on information, opinions, reports, or statements, including financial statements and other financial date, if prepared or presented by:
- one or more officers or employees of the corporation whom the director reasonably believes to be reliable and competent in the matters presented;
- legal counsel, public accountants, or other persons as to matters the director reasonably believes are within the person's professional and expert competence; or
- a committee of the board of which the director is not a member, if the director reasonably believes the committee merits confidence.
- A director is not acting in good faith if the director has knowledge concerning the matter in question but makes reliance otherwise permitted by subsection (B) of this section unwarranted.
- A director is not liable for any action taken as a director, or any failure to take any action, if the director performed the duties of the director's office in compliance with this section.
- Indemnification (To repay for loss or damage):
- Under [RCW 23B.08.520] unless limited by its articles of incorporation a corporation shall indemnify a director.
- Under [RCW 23B.08.570], Section 2, (the corporation may indemnify and advance expenses under [RCW 23B.08.510 – 23B.08.560] to an officer, employee, or agent (e.g., volunteer) who is not a director.
- Under [RCW 2SB.08.560] a corporation may purchase and maintain insurance, on behalf of an individual who is or was a director, officer, employee, or agent of the corporation, against liability asserted against or incurred by the individual in the capacity or arising from an individual’s status as a director, officer, employee or agent.
Meal Reimbursement and Incidental Expenses Policies
Meal Reimbursement and Incidental Expenses Policies (Example)
Meal Reimbursement Policy
- __(insert name of sponsoring organization)__ will only accept:
- Original restaurant meal receipts or
- Original grocery store/convenience store receipts for prepared, ready-to-eat food items that will be eaten by the volunteer driver immediately. Any extra items for spouses or clients will not be reimbursed nor will additional food items be reimbursed, such as cartons of ice cream, canned goods or frozen food items.
- Reimbursement cannot be paid when Supplemental Nutrition Assistance Program (SNAP) funds (previously known as Food Stamps) are used to pay for reimbursable meal expenses at restaurants or for reimbursable ready-to-eat food items purchased from grocery stores/convenience stores.
- All receipts must be have a date and time on them that corresponds to the time span of the authorized trip.
- Receipts for meals will only be reimbursed when volunteering for at least a 4-hour time period. Also, please note that:
- Meals are reimbursed only for the volunteer.
- Meal reimbursements are not authorized for spouses, significant others or clients.
- __(insert name of sponsoring organization)__ does not reimburse for tobacco or alcohol products.
Incidental Expenses Policy
- In addition to meals, __(insert name of sponsoring organization)__ will reimburse for incidental travel expenses related to the non-automobile costs the volunteer incurs. Examples are:
- Parking.
- Highway and/or bridge tolls.
- Ferry tolls.
- __(insert name of sponsoring organization)__ will reimburse for motel/hotel expenses, either pre-authorized, or as a result of weather conditions, delayed/cancelled plane flights, etc.
- In the case of either 1 or 2 above, the expenses must be documented by original receipts.
- Automobile expenses such as: traffic/parking fines, towing charges, gasoline, etc., will not be reimbursed. These expenses are considered to be included in the mileage reimbursement.
I have read and understand the above Policies.
Signature: _______________________________ Date:________________
Rider Grievance Procedure
ABC Transit Customer Complaint Policy (Washington State Example)
ABC Transportation is committed to providing reliable, safe, and satisfying transportation options for the community. Customers of ABC Transportation are a fundamental aspect of our business and as such, their feedback is crucial to the growth and development of the agency.
The ABC Customer Complaint Policy has been established to ensure that riders of the system have an easy and accessible way to provide feedback to the agency. ABC transportation is open to hearing any customer feedback including complaints, comments, suggestions, or concerns.
Contacting ABC Transportation: Riders can contact ABC Transportation in the following ways:
- US Mail: Riders can mail their feedback to the ABC Transportation office at 1 Main Street. Anywhere, [WA 98546].
- Feedback Line: Riders can contact ABC Transportation toll free at xxx-xxx-xxxx. This line is available 24 hour a day, seven days a week
- E-mail: Riders can contact ABC Transportation by e-mail at [feedback@abctransportation.com].
- Fax: Riders can send written feedback by fax to xxx-xxx-xxxx.
- Language Line: For riders who speak a language other than English, ABC Transportation will utilize the services of the AT@T Language Line to facilitate the call.
- Website: Riders can offer feedback on the ABC Transportation Website.
Feedback Review Process: All feedback from customers is valued and will be reviewed by the Customer Service Manager. After review, the Customer Service Manager will distribute the customer communication to the appropriate agency representative(s).
- Customer concerns, complaints, or employee commendations will be forwarded to the appropriate supervisor.
- Recommendations for service or system modification will be sent to the planning department.
- Questions regarding discrimination or bias will be sent to the agency Equal Opportunity Officer.
Feedback Acknowledgement: Anyone who submits a comment, complaint, or service suggestion to ABC Transportation shall receive a response provided they give legible contact information.
- Feedback sent via mail or fax will receive with a response within seven business days.
- E-mail, phone, or web originated messages will be returned with 72 hours.
Customer Appeals Process: Any person who is dissatisfied with the response they receive from ABC Transportation is welcome to appeal the decision. A review team consisting of the General Manager, ABC Customer Ombudsman (may also be County or City ombudsman or customer relations officer); a rider representative and one other staff member will review customer appeals.
Information about Policy: Information about the Customer Complaint Policy, including how to submit a complaint, will be made available to riders:
- When customers are approved for ADA paratransit service
- When customers are re-evaluated for ADA paratransit service or if customers are not re-evaluated, every three years
- On comment cards available on all transportation vehicles
- At the downtown station
- On the website
Reporting: The General Manager shall compile a summary of rider responses for the board, staff, and employees for use in reviewing and evaluating service.
Tracking: ABC Transportation shall maintain a tracking system for all feedback from customers that provides a unique identification of each customer communication and allows ready access to information on the status of the comment at any time.
Protection from Retribution: Customers of ABC transportation should be able to submit feedback without fear of retribution from the agency. If a rider feels like they are being treated unfairly in response to the feedback that they provided, they should contact the ABC Transportation Customer Ombudsman. ABC will appropriately discipline any employee that retaliates against a customer.
Training Standards
Training Standards (Example)
- Program Orientation: All drivers must complete basic orientation training before they transport passengers.
- Vehicle Orientation with Wheelchair Securement and Road Test Training: All van drivers, paid and volunteer, must complete a vehicle orientation, wheelchair securement, and road experience/test training prior to transporting passengers. All drivers using their own vehicles are not required to complete vehicle orientation training but must have road experience/testing prior to transporting passengers. It is recommended that drivers be periodically re-evaluated. This training must be documented in the driver’s Personnel File.
- Certified Defensive Driving Course: All drivers, paid and volunteer, operating a __(insert name of sponsoring organization)__ vehicle or providing transportation in their own vehicle, must complete Defensive Driving Training. The course must be completed within the first six months of driving and repeated every three years for drivers under the age of 70 and every two years for drivers over the age of 70. __(insert name of sponsoring organization)__ offers certified Defensive Driving Instruction (8 hour) and Basic Defensive Driving Instruction (4 hour). A copy of the training certification must be kept in the driver file.
- Disability Awareness: All transportation program drivers and escorts, paid and volunteer, must complete a mobility awareness and assistance training. This course must be completed within the first six months and repeated every three years. A copy of the training certification must be documented in the driver file.
A copy of the certifications of completion for these courses must be kept in the driver/escort’s file.
Recommended Supplemental Training (not required):
Certified CPR/First Aid Training
Commercial Drivers License (CDL) (For van drivers)
Customer Service Training
These training requirements apply to all volunteer driver programs.
Waivers, Agreements To Participate, & Hold Harmless
Waivers, Agreements To Participate, and Hold Harmless* (Example)
*Forms and policies should always be reviewed by your legal counsel to ensure compliance with state and local laws and for liability purposes.
- RELEASE: A Release or waiver excuses the provider of a service from responsibility from their duty to protect the participant. It is an exculpatory agreement that releases the provider from duty owed. A Release is signed prior to the service being provided. The Release is a contract between the participant and the provider organization that the participant, for consideration (payment and/or the ability to participate) will not sue for damages or injuries. The Release can include an agreement not to sue even for the negligence of the provider.
- Courts examine certain criteria before holding a Release to be valid:
- The Release must be signed by a participant of majority age. Since minors cannot contract they cannot legally enter into a Release agreement. Parents cannot sign for a minor, but they can sign for themselves, on their own behalf, and this would hold.
- There must be alternatives available to the potential participant.
- The Release must be voluntarily signed, that is, it must not be an adhesion contract.
- The adult signing the Release must be mentally competent.
- The language of the Release must be very clear, explicit, without ambiguity, and printed in an obvious place, that is, not hidden in small type.
- AGREEMENT TO PARTICIPATE: An Agreement to Participate (ATP) or Assumption of Risk (AR), goes to two legal concepts, assumption of risk and contributory negligence. The ATP is not a contract, it is a signed acknowledgment that the participants understand all the dangers, inherent in the activity or program, that they know the rules, and that they appreciate the risks that could result from participation.
- An effective ATP will have several criteria:
- Must be explicitly worded.
- If there are rules that must be followed, it is preferable that the rules be listed in the agreement or listed on the reverse side of the paper.
- The possible dangers inherent in the activity, including dangers from other passengers and/or equipment, must be spelled out in detail along with the potential consequences.
- The ATP must be signed.
- When transporting a minor child, or incompetent adult, an effective practice would be for the Release to be signed by the parent or legal guardian and the Agreement to Participate to be signed by the minor. This is a good combination and affords protection to the Sponsoring Organization.
- HOLD HARMLESS: An Indemnification Agreement (IA), and/or Hold Harmless Agreement (HHA) are methods of protecting staff, volunteers, and agencies from financial loss in the event of a judgment against them. An IA comes into action after an award has been made. If a participant signs an IA, is injured, sues for negligence and is awarded recovery, the Agreement comes into force. The Agreement causes the plaintiff to reimburse the defendant for the amount of the recovery. The effect is that there is no payment. The Indemnification Agreement will not help against an insolvent client if the provider is sued by a third party not bound by any agreement.
- GENERAL INFORMATION: Private enterprises can use the Release successfully. Public agencies cannot depend on a Release for defense because it may be contrary to public policy: however, an Agreement to Participate and a Hold Harmless Agreement are useful for a public agency.
- The use of signature forms is not suggested for fixed-route transit services; although they can be used with a specific group trip, e.g., a charter, particularly if the group is considered difficult to transport. Releases, and other legal forms, are extremely useful for specialized one-on-one transportation services provided by paid or volunteer staff using private or agency owned vehicles. Regardless of the particular circumstances they should be used for any transport considered high-risk, or non-routine.
- A Driver Release section is included in the Volunteer Transportation Release form. In order for any specialized transportation provider to deliver reasonable and prudent, professional service, the legally required standard, the driver must have the right to refuse to provide the service. For the Driver Release to hold, the driver must sign voluntarily which means that the driver will not suffer adverse consequences for making a reasonable and prudent professional decision.
- The service provider must have a "Policy On Refusing Service,” based on the staff's judgment of the situation rather than on rules. For example, service would not be refused because a potential rider was in an unfamiliar, difficult to secure, wheelchair. Instead, a Release could be used to protect the service provider. In contrast, an obviously drug influenced, hostile person would be refused service based on the driver's professional judgment. A specialized transportation service provider faces many situations of potential liability if the driver is not appropriately trained and expected to exercise professional judgment. Rules and policies cannot substitute for judgment; they only can supplement judgment.
Sample Forms (Examples and Templates)
Adult Protective Services Reporting Form
Adult Protective Services Reporting Form (Example)
Identification of Individual(s)
Name: ____________________ Address: _________________ Telephone: ________
Identification of Suspected Perpetrator(s)
Name: ____________________ Address: _________________ Telephone: ________
Relationship to Individual Being Reported:
Son Brother Spouse Son-in-law
Daughter Sister Caregiver Daughter-in-law
Father Mother Other
Description of Suspected Abuse/Exploitation/Neglect or Abandonment (Use back of report if needed.)
Identification of Significant Others: (if known)
Name: ____________________ Address: _________________ Telephone: ________
Agencies Currently Providing Services to Individual(s) (if known)
Name: ____________________ Address: _________________ Telephone: ________
Source of Report:
Reported by: (name): _____________________ Date of Oral Report: _____________
Agency: _________________________
Relationship to Individual Being Reported ________________________________
Report to:
Back-Up Plan for Daily Operations with Sample Emergency Card
Back-Up Plan for Daily Operations (Example)
In the event of a collision or mechanical breakdown, the driver will contact the dispatch center or the manager and inform of incident. Driver will place proper hazard equipment in the appropriate locations to alert other drivers of his/her position. The driver will remain with the vehicle and passenger(s). If possible, the vehicle will be moved to a safe location until assistance arrives. Follow appropriate collision procedures in the event of a collision.
Dispatch Center Phone #s: _______________________________________________
Towing Company: ________________________________ Phone: ______________
Repair/Service Company: __________________________ Phone: ______________
Manager or Dispatch Staff will: *
- Contact towing company to remove vehicle and deliver to designated location.
- Contact location where vehicle is to be towed for repairs/service.
- Contact driver and update him/her of who is coming and approximate time of arrival.
- An alternate driver and vehicle is dispatched to pick-up passengers and deliver them to their destination.
- Adjustments are made to the schedule to assure passengers are delivered safely to their final destination.
- Arrangements are made for the driver to return to dispatch after the vehicle is removed.
* Note: This is meant to only serve as a sample to develop your back-up plan specific to your program. Your back-up plan should include names and phone numbers to contact and more in depth plans. All of this information should be laminated onto a Driver ID number.
Sample Emergency Card:
Emergency Numbers: In case of emergency, please phone:
During the Week (8:00 to 5:00), __(insert name of sponsoring organization)__ Office(s):
Ask for: _______________ Name of Manager: ________________
Evenings or Weekends:
Name: ______________________ Phone: ___________________
Name: ______________________ Phone: ___________________
Name: ______________________ Phone: ___________________
If no one is at home, call “The Line”: Phone: __________________
Remember, in the case of accident, Call the Police.
Back-Up Plan for Vehicle Loans or Out-of-Area Service
Back-Up Plan for Vehicle Loans or Out-of-Area Service (Example)
[Date]
[Name of Borrowing Program]
[Address]
[City/Town, State Zip Code]
Attention: [Manager of Borrowing Program]
On (Date of Trip),
__(insert name of sponsoring organization)__ has authorized [Name of Borrowing Program], to travel to [Destination]. The driver will be [Name of Driver] and has been approved and trained to transport passengers.
In the event that an unforeseen collision or mechanical breakdown was to occur, the driver should phone [Name of On-Call Person]. The __(insert name of sponsoring organization)__ back-up vehicle would retrieve the passengers and return them safely home. __(insert name of sponsoring organization)__ will arrange for the vehicle to be towed back to the provider site or to an alternate location for repairs.
If you have any questions regarding this trip please contact [Name of Contact] at this phone number [Phone Number(s) of Contact].
Sincerely,
[Name of Person Responsible for Back-Up Plan]
[Position of Person Responsible For Back-Up Plan]
Volunteer Driver Availability
Volunteer Driver Availability (Example)
Name: __________________________________
Please check the boxes below for the days of the week you would be interested in volunteer driving, including weekends and holidays. If there are certain time periods in which you wish to volunteer, please note. If there are particular regular dates of the month you are not available then note them in the
Comments section below.
| Day of the Week | Yes | No | Restricted Times of the Day or Daylight Only |
|---|---|---|---|
| Sunday | |||
| Monday | |||
| Tuesday | |||
| Wednesday | |||
| Thursday | |||
| Friday | |||
| Saturday |
Comments:
__(insert name of sponsoring organization)__ attempts to estimate the approximate length of client appointments, but realize that doctors can request more tests or procedures. Please be patient and if you think that you are going to be short on time, do not accept the ride request.
Below, please list any trips that you may not be interested in accepting. Most client medical information is confidential. __(insert name of sponsoring organization)__ is not routinely allowed to release the medical reason for appointments. The dispatch center will have this information. There may be some trips that you would prefer not to accept; for example, trips to dialysis, mental health appointments, family planning clinics, etc. Please note if you feel uncomfortable transporting certain ages and/or persons of a different sex. Note if you are comfortable with using car seats and willing to be trained.
Name: ____________________ Signature: ________________ Date: _____________
Driver Evaluation
Driver Evaluation (Example)
Driver Medical/Physical Release
Volunteer Driver Medical/Physical Release (Example)
I verify;
I do not verify;
That (name): ______________________ is physically capable of operating a personal automobile for the purpose of providing volunteer transportation for individuals eligible for this service.
In addition, I have reviewed all prescription and/or over-the-counter medications currently being taken by the above individual. I have no concerns regarding their use while (name):_____________ is operating a motorized vehicle.
Physician’s Name: _______________________________________________
Address: ___________________ City/Town: _____________ State: ____ Zip: ______
Phone: _______________________ Email: ________________________
Physician Signature: _________________________ Date: ________________
Please return this form directly to:
__(insert name of sponsoring organization)__: ________________________________
Address: ___________________ City/Town: _____________ State: ____ Zip: ______
Phone: _______________________ Email: ________________________
Driver Reference Form
Volunteer Driver Reference (Example)
Name of Volunteer Applicant: _________________________________________
Name of Reference: _________________________________________________
Address: ________________________________ Phone: ___________________
CIRCLE OR CHECK ALL THAT APPLY FOR EACH QUESTION
1. What is the nature of the relationship with this applicant? (Check all that apply)
employer ___ friend ___ neighbor ___ family friend ___ counselor ___
teacher ___ relative ___ coworker ___ other
2. How long have you known the applicant? __________________________
3. How well do you know this person? very well ___ fairly well ___ acquaintance ___
4. Volunteers will be required to keep confidential any information given about a client. In your experience, have you ever known him/her to keep things confidential?
__________________________________________________________
5. How would you describe this person’s style with people?
sincere ___ shy ___ shallow ___ distant warm ___ demanding ___ caring ___
consistent ___ accepting ___ judgmental ___ indifferent ___ patient ___
don’t know ___
6. Do you feel the applicant would be compassionate and caring to the following populations? Check all those that you feel would apply:
mentally challenged ___ physically challenged ___ behaviorally challenged ___
low income ___ older adults ___ Non-English speaking___
7. What is the applicant’s relationship with young children?
communicates effectively ___ mild conflict ___ over protective ___
caring ___ much conflict ___ don’t know ___
8. How would you rate the applicant’s relationship with teenagers?
friendly __ has “Generation Gap” __ understanding __ impatient __ patient __
lacks confidence __ well-liked __ stern __ accepting __ don’t know
9. Would you trust the applicant with your own child or a child close to you in an unsupervised setting? Yes ___ No ___ If No, please explain:
__________________________________________________________
10. Do you believe that the applicant has the moral character necessary to transport a child without supervision? Yes ___ No ___ If No, please explain:
11. Check as many of the following that describe the applicant:
confident __ nervous/tense __ outgoing __ sense of humor __ responsible __
temperamental __ judgmental ___ friendly __ unreliable __ flexible
12. Does this person deal well with the responsibilities and problems of everyday living?
almost always ___ usually ___ sometimes ___ rarely ___
13. In your experience as a passenger in the applicant’s vehicle, have you found him/her to be a safe and cautious driver?
_________________________________________________________
14. How would you rate this person’s health?
excellent ___ good ___ poor ___ some problems ___
15. Please describe this person’s strengths and weaknesses:
Strengths:
__________________________________________________________
Weaknesses:
__________________________________________________________
16. Does this person have or ever had a drinking or drug abuse problem?
__________________________________________________________
17. Has this person ever been arrested for an illegal activity, including drugs or DUI?
__________________________________________________________
18. Do you know any reason why this applicant would not serve well as a volunteer driver?
_________________________________________________________
If you have any additional information or comments about this applicant that you would like to share with us, please feel free to call at: ____________ Ask for: _________
Thank you for your cooperation!
Signature: ________________________ Date: ___________________
Driver Road Test
Volunteer Van Driver Road Test (Example)
Driver Statement of Medical Condition
Volunteer Driver Statement of Medical Condition (Example)
Below is a checklist of certain conditions, the drugs commonly prescribed, and their potential side effects on driving. Check any that apply to you and describe below your condition, level of medication, the effects it has on your driving, and any other comments relative to how your physical or emotional condition and/or drugs taken influences your ability to drive safely. Then sign in the space below.
If you have no physical or emotional conditions that impair your driving and are currently taking no drugs that impair your driving, simply sign and date this page below. The information you provide will be kept confidential as required by the Privacy Act. Based on the information provided, __(insert name of sponsoring organization)__ may request a physician’s release prior to authorizing volunteer driving.
Comments:
Name (Print): __________________ Signature: ______________Date: _________
Driver Statement of Understanding
Volunteer Driver Statement of Understanding
(Washington State Example)
The purpose of the volunteer driver is to provide safe and reliable transportation to and from essential services (e.g., medical facilities, social services, nutrition sites, etc.). Volunteer drivers in this program drive their own cars and may, or may not, be reimbursed for expenses incurred. Only expenditures that have been requested by __(insert name of sponsoring organization)__ will be considered for reimbursement. __(insert name of sponsoring organization)__ provides general liability insurance for the overall program and covers the volunteer driver with state medical insurance.
The rider being transported by a volunteer driver is a person who has been determined by __(insert name of sponsoring organization)__ to have no appropriate means of personal transportation available.
[The following minimum insurance coverage is required by the State in the Code of WA (RCW 46.29.090): $25,000 bodily injury, each person: $50,000 bodily injury, each accident: $10,000 property damage.]
I understand that I must meet these standards for motor vehicle insurance, policy, or bond. My personal insurance is the primary liability protection and must be issued by a company authorized to do business in my state of residence.
I will provide proof of coverage of my vehicle insurance. In the event that my coverage changes or is canceled, I will immediately notify __(insert name of sponsoring organization)__ of such changes or cancellations.
I have had a valid driver’s license for the past five (5) years. I will provide a copy of my valid driver’s license. I understand that the (Sponsoring Organization) will be requesting a State Patrol Identification History Check.
I have had no at-fault vehicle accidents in the past three years and agree to have __(insert name of sponsoring organization)__ verify my driving record. I will notify immediately & provide __(insert name of sponsoring organization)__ with a copy of:
- A report in the event I am involved in a vehicle accident.
- Any traffic citation that I may receive while this agreement is valid.
I am physically capable of driving my vehicle safely and will not drive while using any drug that may affect my driving ability, either prescription or “over the counter.” If requested, I will provide a statement from my physician stating that I am capable of participating in this program.
My vehicle is mechanically sound and is equipped with seat belts which I will use and enforce use by my passengers. Children aged 12 & under will be placed in the rear of the vehicle & child restraint (seats chairs) will be properly used for all children under 3 years or 40 lbs. __(insert name of sponsoring organization)__ will provide appropriate child restraint equipment.
I will maintain all records required by __(insert name of sponsoring organization)__. I will not accept donations from riders, but will encourage riders to make any donation directly to __(insert name of sponsoring organization)__.
I will protect the rider’s right to confidentiality. I will also respect their right to pursue an independent lifestyle, and be non-judgmental in my interactions with them.
I have been provided with information about __(insert name of sponsoring organization)__, the purpose of the Volunteer Transportation Program, and my role as a driver and responsibilities.
I will notify __(insert name of sponsoring organization)__ at the time I no longer wish to be involved in this program. Either __(insert name of sponsoring organization)__, or I, may terminate this agreement at any time.
I have read and understand the above statements.
Signature:_________________________________ Date: ______________
Driver Training Checklist
Driver Training Checklist (Example)
Driver’s Name: _________________________ Driver Application Date: _______
DOB: _____________ Program Orientation Date: _________
Driver Type: Agency Vehicle: __ Personally Owned Vehicle (POV): __ Combination: __
Insurance Confirmed:
_____________
Exit Interview
Exit Interview (Example)
Name of Volunteer Driver: ________________________ Date: ___________
Name of Interviewer: __________________________________
1. Did the position match the work you desired?
2. Why have you decided to leave your position?
3. How would you describe your relationship with other volunteers and/or paid staff?
4. How would you describe your relationship with program staff?
5. What did you like most about your experience?
6. What was the hardest part of the job?
7. What recommendations for change would you make?
8. Would you recommend this opportunity to others?
9. Is there any other information that you would like to provide?
10. Would you consider volunteering for the (Sponsoring Organization) in the future?
Exposure Incident Report
Exposure Incident Report (Example)
Use this form to report any bloodborne pathogen exposure incidents. An exposure incident is a specific contact of blood or other potentially infectious bodily fluid with non-intact skin, eye, mouth or other mucous membranes.
Date and time of exposure: _____________________ Report Date: _________
Name (person exposed): _________________________________________________
Address: ___________________________ Phone: ________________________
Agency: ______________________________________________________________
Name of Customer (Source of bodily fluid): ___________________________________
Address: ____________________________ Phone: ________________________
Name(s) of witnesses: ____________________________________________
Part of body exposed to bodily fluid: ________________________________________
Type of bodily fluid: _____________________________________________________
Describe incident: _______________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Treatment received at: _______________________________________________
Name of physician: __________________________________________________
Employee/volunteer signature: ___________________ Date: _______________
Supervisor signature: __________________________ Date: _______________
Action taken: ______________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Email form to: (Email address of
__(insert name of sponsoring organization)__)
FBI Fingerprint Form (Sample)
FBI Fingerprint Form (Sample)
The FBI does not allow copies to be submitted. An actual FBI Form 258 has to be used. These forms either can be ordered in bulk or secured from local law enforcement officials.
Front of FBI Form 258
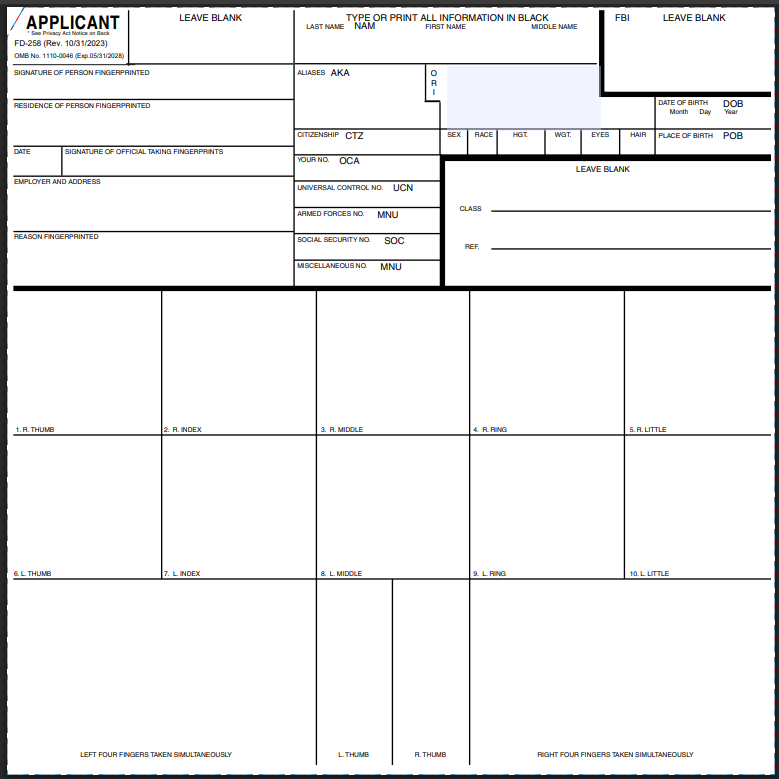
Back of FBI Form 258
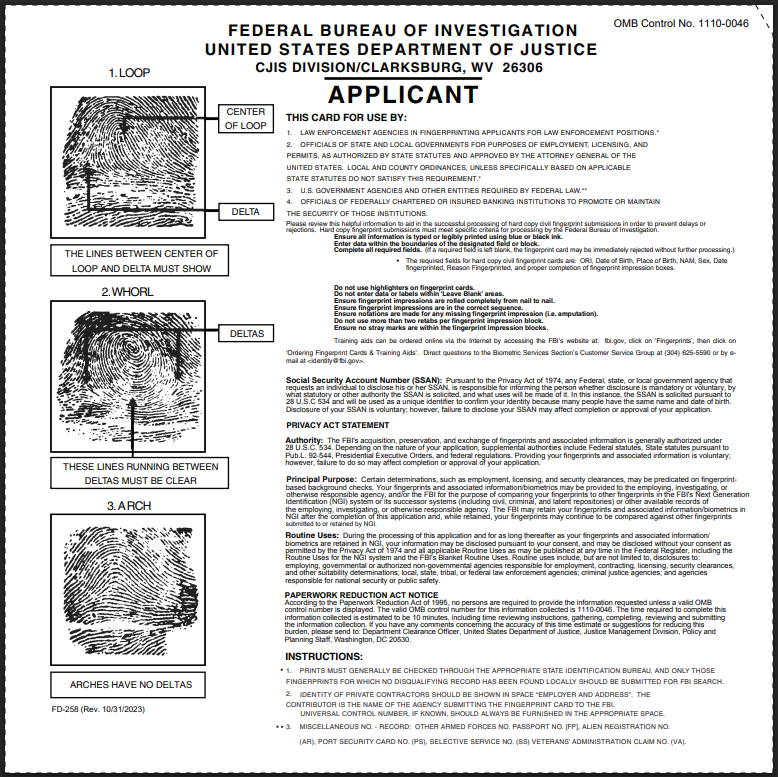
Incident & Collision Report
Incident & Collision Report (Example)
Accident: ____ Incident: ____
Date:
__________
Time: _________ Region #: ____________ County: ___________
Medical Treatment: Yes or No
Injuries: Yes/No 911 Called: Yes/No ER Visit: Yes/No Admitted: Yes/No
Driver Sent for Drug and Alcohol Testing: Yes/No Test Results: ___________
Client Name: ________________ PIC: ______ Non-Ambulatory: ___ Ambulatory: ___
Accident/Incident Narrative: _______________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Insurance Company Name, Contact, Policy # _________________________________
(Attach Additional Documentation)
Driver Report: __ Dispatcher Report: __ Broker Report: __ Other: __
FOLLOW-UP:
Date: ____________
Driver Status: Terminated: ____ Suspended: ____ Re-trained: ____ Other: ____
Narrative: ______________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Client or Advocate Re-Contacted: Date: ______________
Narrative: ______________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
No follow-up required; investigation closed:
Date: ___________ Initials:______
Incident Report – Volunteer Driver
Volunteer Driver Incident Report (Example)
- Driver Name: ________________________________________________________
- Date of Incident: __________________
- Time of Incident: __________________
- Location of Incident: __________________________________________________
- Name of Rider(s) Involved: _____________________________________________
- Address: ___________________________________________________________
- Phone Number: ____________________ Authorization Code: ________________
- Car Seat or Booster Seat in Use? ________________________________________
- Name & Phone Number of Witnesses to Incident:
Name & Phone: ______________________________________________________
Name & Phone: ______________________________________________________
Name & Phone: ______________________________________________________
- Explain in Detail: ____________________________________________________
______________________________________________________________________
PLEASE FILL OUT THIS FORM COMPLETELY AND MAIL TO:
Lift Operation Procedures and Checklist
Lift Operation Procedures* and Checklist (Example)
Wheelchair lifts make it possible to load wheelchairs of all weights in an efficient and safe manner. However, lifts are potentially hazardous equipment. They must be maintained and operated properly. Considerable caution and awareness is needed when operating a lift. No one but the vehicle operator should operate the vehicle wheelchair lift. Lifts may differ slightly in structure and operation. Therefore, each vehicle operator should be familiar with all the lifts likely to be used. __(insert name of sponsoring organization)__ may have specific policies pertaining to wheelchair lift operations. It is recommended that you check with your manager or supervisor concerning these policies.
*What follows is general information and guidance for lift operation procedures. Programs should ensure that current policies and procedures agree with manufacturer’s guidelines for the securement systems currently in use. For more information about where to find training for volunteer drivers, see Section 4 – Establishing and Managing a Volunteer Driver Pool.
Loading Riders Who Use Wheel Chairs: Checklist
- Upon arriving at your destination:
- Stop on level ground. □
- Make certain there is room for the lift platform to open without hitting obstacles. □
- Put vehicle in Park, not Neutral.
The lift will not work if the transmission is in Neutral. □ - Set the parking brake. □
- Opening doors:
- Open lift doors from outside vehicle. □
- Securely lock doors in open position. □
- Deploying the lift:
- The lift is always operated from the ground. □
- Do not remain in the vehicle while raising and lowering the lift platform. □
- Lower the lift platform until it rests entirely on the ground. □
- Unfold the outboard roll stop. □
- Fasten the wheelchair seat belt around the rider. □
- Interacting with passengers and getting onto the lift platform:
- Greet passengers; talk to them, not around them. □
- Ask passenger if they would like assistance in getting onto the lift platform. □
- If lift is ADA approved, the passenger may ride on the lift facing the van. □
- If the lift is not ADA approved, explain the potential hazard and request that the passenger ride on the lift with their back to the vehicle.
Remember, under the ADA, it is the rider’s choice. □ - If the lift is equipped with a safety belt make certain that it is attached and secure. □
- Lift operation:
- Set the wheel chair locks. □
- Have the rider hold on the handrails if able □
- Remind the rider to keep arms and hands within the lift area and clear
of moving parts. □ - Stand on ground with one hand on the wheelchair and one hand operating
the controls. □ - Raise the platform only a couple of inches. □
- Check the front safety barrier to make sure it is locked. □
- Continue raising the lift platform to the floor level. □
- Transferring to the vehicle:
- Put lift controls in secure position with one hand while holding onto the
wheelchair with the other. □ - Release the wheelchair wheel locks. □
- Push the wheelchair into the van. □
- Reach in and lock the wheels. □
- Fold the lift into the travel position and shut the doors. □
- Unloading: Use a logical reversed sequence for unloading.
Notes on power chairs and scooters - Caution is needed when loading a power wheelchair onto a lift. If the chair’s power is left on, there is potential for the chair to move while on the lift, even if the brakes are applies. Many individuals operating these chairs are slow in reaction, or may have involuntary movements which may cause their hand or arm to hit the control stick. It is recommended that the power sources be disengaged while lifting a power wheelchair.
Boarding standees on the lift - The ADA allows anyone who wishes to board the vehicle standing on the lift. The procedures for loading a standee are similar to those used for boarding a person in a wheelchair. With an ADA approved lift the person should board facing inward after the roll stop has been lowered. The person should be encouraged to let go of any mobility device like a walker and to grasp the hand rails. The safety belt, if there is one, should be secured behind the standee. Once the lift is in level with the floor of the van, the standee should be instructed to move into the vehicle.
Walking Aids - When transporting people who use walking aids, it is the driver’s responsibility to store the walking aid in a safe and secure place. Ask the passenger if there is a special way they would like the walking aid to be handled. If a passenger is using a cane, they may prefer to keep it with them.
Manual operation of the lift - Most lifts are equipped with a hydraulic pump located within the plastic motor housing on the side of the lift. A steel pump arm is found on the outside of the housing or the lift frame.
- Lowering: To lower the platform manually, turn the bleeder valve, located near the pump opening, just enough to allow the platform to drop slowly. Do not unscrew it too far or hydraulic fluid will leak. When the platform has reached the ground tighten the valve.
- Raising: To raise the platform, insert the pump arm into the pump opening. Pump the arm. The platform will rise very slowly.
Personnel Checklist
Personnel Checklist (Example)
Pre-Trip Inspection and Checklist Form
Pre-Trip Inspection (Example)
1. Conducting the Inspection: Before you begin, you should have a copy of the checklist in hand and have a pen to write with. The checklist will help you in performing the inspection in a logical sequence and assist you in doing a complete and thorough inspection of the vehicle. If your vehicle does not contain all of the equipment that is reflected in the checklist, i.e., organization van vs. personally owned vehicle (POV), simply cross out the items that do not apply and move on to the next item.
2. Fluid Levels, Hoses, Belts: Before you start the engine, lift the hood. Check the fluid levels in the radiator, battery, and windshield washer. Note any excessive usage and add the appropriate fluids. Check the oil level and add if indicated. Note any of the fluid additions.
Visually check the hoses for signs of leaking and/or cracking. In a similar way check the belts.
3. Interior, Lights, Dials, Gauges and Ventilation: Once you get behind the wheel, set the emergency brake, start the vehicle, check the appropriate lights, dials, and gauges. For example, the oil gauge or warning light should give you an indication as to whether the oil pressure is sufficient to keep the engine running without damaging it. Do not allow the engine to “race” when you first start it. If the engine seems to be running too fast (idle,) and will not slow down, do not put it into gear. Shut it down and report the problem to the manager.
If the alternator or generator light stays on or if there is a gauge that tells you the battery is not charging, you could end up with a dead battery on the route. If you do get such an indication you should have it corrected before starting out on your assigned trip.
Check to see if heater and air conditioning are working. Notice any foreign smells coming from the ventilation system. Inspect the interior for any hazards, torn upholstery, loose objects, etc. Check the interior lights, and seat belts. If car seats or other child restraint systems are to be use, check to determine if they are matched to the vehicle and that they can be properly activated. Note the presence of driver side airbags in planning for the anticipated passengers, i.e., if they are present and activated then children and small adults should not ride in positions with functioning air bags.
Check for the vehicle registration and proof of insurance; make sure that neither has expired. Check for presence of EZ Clean Kit in the vehicle. Check supplies in the kit.
4. Windows and Mirrors: Make sure that all windows and mirrors are free of ice, snow, or frost before moving the vehicle. If it is not too cold outside, you can check to see that the windshield washer and wipers are working.
Adjust all of your mirrors to make sure that you can see what it is you need to see within your safety zone.
5. Horn, Steering Wheel, and Brakes: Tap the horn to make sure it works.
Move the steering wheel from side to side to make sure that it does not have excessive “play” in it. Push on the brake pedal. It shouldn’t feel soft or spongy.
6. Doors and Emergency Exits: Examine all regular and emergency doors to make sure that they are functional and not obstructed or otherwise damaged. The time to find out that an emergency door does not work is before the vehicle is put into service.
7. Left Front: Turn on all the exterior lights, including the high beams, turn signals and emergency flashers. Make sure the emergency brake is on and get out and check the left front vehicle lights to make certain that they are clean and not burned out. As you begin this outside inspection, remember to note any new damage to the vehicle.
8. Left Side Tires: Look at the left front and left rear tires for signs of damage or obvious pressure problems. An over inflated tire will give a rougher ride. An under inflated tire will build up heat and make it more susceptible to damage from obstacles or potholes in the road. If you have a tire gauge, check the pressure against recommended levels.
9. Trunk, Rear Lights, and Signs: Check in the trunk, interior, or under the vehicle for the spare tire and tire changing tools. Check inflation of the spare. Check for presence of an emergency equipment kit (chains, flashlight, flares, blankets, ice scrapers).
Inspect all lights on the rear of the vehicle such as the emergency flashers, taillights, etc. If there are any signs on the back of the vehicle make sure that they are clean. If lights are dirty clean them.
Check to determine if the license tabs have expired.
10. Under Vehicle Inspection: Stand back a few feet from the rear of the vehicle and look under the vehicle or any foreign objects or fluid leaks. If there any objects hanging or wedged under the vehicle, either remove them or determine if part of the vehicle is hanging down. If a part of the vehicle is hanging down, report it to the manager for repair before starting your run. If you see any puddles of any kind other than obvious rainwater or water from melted snow/ice, check the source of the leak and report it to the manager.
11. Right Side Tires: Now check the right rear and right front tires just as you did the tires on the left side. Again, look for any signs of fresh vehicle damage.
Pre-Trip Inspection Form
Pre-Trip Inspection Form (Example)
Private Vehicle Registration
Private Vehicle Registration (Washington State Example)
Name: ________________________________________________________________
Address: _______________________ City/Town: ________________ Zip: __________
Phone: _______________________ E-Mail: __________________________________
Vehicle(s) #1 Make: _____________ Year: ____________ Air Bag(s): ______
Model: _____________ Color: ______________ Seating: ________
License #: _______________________
#2 Make: _____________ Year: _____________ Air Bag(s): ______
Model: _____________ Color: ______________ Seating: ________
License #: _______________________
Insurance Company: _____________________________________________________
Insurance Agent: ________________________________________________________
Address ________________________ City/Town: _____________ Zip: ___________
Telephone: _______________
I certify that I am currently insured through the above company for automobile liability insurance in an amount in excess of or equal to the minimum required under [Washington State law. (Liability: $100,000 per individual/$300,000 per occurrence/Property Damage: $50,000 per occurrence).]
Further, I agree to forward a photocopy of my Proof of Insurance Card at each renewal period.
Further, I agree to immediately notify __(insert name of sponsoring organization)__ in the event that the above liability insurance is revoked, cancelled or altered in such a manner as to no longer meet the minimum vehicle insurance requirements for the State of [Washington].
Further, I agree not to a transport any passengers as part of the volunteer driver program if these minimums liability requirements are not met, or if my [Washington] vehicle operator’s license is not current and/or valid, or if the registration and license of the vehicle (s) I use to transport passengers is not current and/or valid.
Further, I certify that my vehicle(s) is in safe operating condition.
Further, I agree to hold harmless and indemnify __(insert name of sponsoring organization)__, the manager, and the passenger(s) against any or all claims arising, all or in part, from my negligence.
Further, I authorize __(insert name of sponsoring organization)__ to make periodic checks of my driving and criminal record.
Signature: ______________________________________Date: __________________
Rider Registration/Trip Request
Rider Registration/Trip Request (Example)
MUST BE FILLED OUT COMPLETELY SUBMIT REQUEST TO: (Program Contact)
Riders Name: ____________________________ Billed to: __________________
Address: ___________________________________ Birthdate*: ______________
City: __________________________________ State: ___________ Zip: ________
Phone: __________________________________ Email: ____________________
Does rider have any other transportation available?: ____________________________
Live Alone: Yes ___ No ___ Low Income: Yes ___ No ___ ID#: ___________
Medicaid: Yes ___ No ___ Minority: Yes ___ No ___ ID#: __________
Understands English: Yes __ No __ Program Eligibility: ____ Race Code: _______
Have we worked with Rider Before?: Yes __ No ___ Sub-Allocation: ___ Billing: ____
Single Parent Household: Yes ___ No ___ Social Security Number: ___________
Ambulatory; Wheelchair; Walker; Attendant; Other: ___ Disabled Placard: __________
Contacted by: _____________________________ Phone: __________________
Out of Area: ________ Referring. Physician.: ______________ Phone: __________
*If age is below six (6) years: Height: _____________ Weight: ____________
Directions/Comments:
______________________________________________________________________
______________________________________________________________________
Entered in database by (Initials): ___________
Trip Date: ________ Car Seat Required: Yes __ No __ Booster Seat: Yes __ No __
Appointment Time: ________ Pick Up Time __________ Return Time: _____________
Physician: _____________________ Doctor or Clinic Phone: ____________________
Address: ______________________________________________________________
Purpose: ______________________________________________________________
Provider Recommended:________ Provider Chosen: ________ Phone: ___________
Estimated Mileage: ________ Called Rider To Confirm Ride: ____________________
OFFICE USE ONLY:
Intake by: _________ Date: ________
Additional Information:
Completed by: _________ Date: ________
Voucher Mailed by: _________ Date: ________
Transportation Request
Transportation Request (Example)
MUST BE FILLED OUT COMPLETELY
Riders Name: _________________________________ Billed to: _________________
Address: _____________________________________ Birthdate*: ______________
City: ________________________________ State: _____________ Zip: ________
Phone: ____________________________ Email: ___________________________
Does rider have any other transportation available?: ____________________________
Live Alone: Yes __ No __ Low Income: Yes __ No __ ID#: __________
Medicaid: Yes __ No __ Minority: Yes __ No __ ID#: __________
Understands English: Yes __ No __ Program Eligibility: _____ Race Code: ______
Have we worked with Rider Before?: Yes __ No __ Sub-Allocation: ___ Billing: ____
Single Parent Household: Yes __ No __ Social Security Number: ___________
Ambulatory; Wheelchair; Walker; Attendant; Other: ____ Disabled Placard: ________
Contacted by: _____________________________ Phone: __________________
Out of Area: ________ Referring. Physician.: _______________ Phone: _________
*If age is below six (6) years: Height: _____________ Weight: ____________
Directions/Comments:
______________________________________________________________________
______________________________________________________________________
Entered in database by (Initials): ___________
Trip Date: ________ Car Seat Required: Yes __ No __ Booster Seat: Yes __ No __
Appointment Time: ________ Pick Up Time __________ Return Time: _____________
Physician: _____________________ Doctor or Clinic Phone: ____________________
Address: ______________________________________________________________
Purpose: ______________________________________________________________
Provider Recommended:________ Provider Chosen: _________ Phone: __________
Estimated Mileage: ____________ Called Rider To Confirm Ride: ________________
OFFICE USE ONLY:
Intake by: _________ Date: ________
Completed by: _________ Date: ________
Voucher Mailed by: _________ Date: ________
Additional Information:
Trip Description
Trip Description (Example)
The purpose of the following agreement is to provide the framework for better understanding among all the participants involved in the transportation described below.
To be completed by the staff of __(insert name of sponsoring organization)__:
Rider’s Name: _________________________________ Phone: __________________
Address: ___________________________ City/Town: _______________ Zip: _______
Physician’s/Nurse’s Name: _______________________ Phone: __________________
Address: ___________________________ City/Town: _______________ Zip: _______
Trip Destination: ________________________________ Phone: _________________
Address: ___________________________ City/Town: _______________ Zip: _______
Approximate distance and length of time for travel: _____________________________
Special Instructions/Directions:
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Trip Purpose:
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
If for hospital admission, has admitting office been notified? Yes: ___ No: ___
Further instructions:
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Vehicle used: Organization Van: ____ Private Auto: ____
Trip Voucher
Trip Voucher (Example)
MONTH: __________ VOUCHERS DUE IN OFFICE BY THE ___ OF EACH MONTH
I hereby certify that this account of travel is accurate.
I am requesting reimbursement: YES: _ NO: _
TOTAL MILES: _____ X $. _____ = $ ______ Report Incidental Expenses Above: _________
SIGNATURE OF VOLUNTEER DRIVER: __________________________ DATE: _________
VOLUNTEER NAME (Print): _________________________
ADDRESS: ____________________ CITY: _______________ STATE: __________ ZIP: ____
PROGRAM CODES: (OFFICE USE)
Volunteer Driver Job Application
Volunteer Driver Job Application (Washington State Example)
This application will be used to establish your eligibility as a volunteer driver for __(insert name of sponsoring organization)__. The information you provide helps us assure you, this organization, and the public that the highest standards of safety and accountability are maintained. We appreciate your cooperation and interest in our volunteer driver program. Return completed application to your __(insert name of sponsoring organization)__ Vanpool Coordinator.
Application for: Volunteer Personally Owned Vehicle (POV) Driver: ___
Volunteer Van Driver: ___ Combination: ___
Volunteer Transportation Program Client Survey
Volunteer Transportation Program Client Survey (Example)
Name: ______________________________________ Date: _________________
Address: ____________________________________ Phone: ________________
What was the name of the driver who transported you?__________________________
How can we improve service to you?________________________________________
(Please use additional paper if needed)
Please Return the Survey to:
Program Manager:
__(insert name of sponsoring organization)__:
Address:
Volunteer Transportation Release
Volunteer Transportation Release (Example)
1. Rider: (Indicate appropriate responses and sign)
The undersigned assumes all reasonable risks involved in this round-trip. The length of the trips, both miles and time, has been explained to me. The vehicle to be used has been explained to me. I know that the driver (Name), has / does not have first aid and CPR training. The driver has / does not have special training in passenger assistance techniques.
The undersigned understands and expressly assumes all the dangers of the round-trip. The undersigned waives all claims arising out of the transport whether caused by negligence, breach of contract or otherwise, and whether for bodily injury, property damage or loss or otherwise, that I may ever have against __(insert name of sponsoring organization)__, its successors and assigns, and its officers, directors, agents (e.g., volunteers), and employees, and their executors, administrators and heirs.
Signed: _________________________________ Date: ________________
2. Physician/R.N: (Please sign/R.N. sign following telephone authorization.)
There is no reason or condition that may cause the above named person difficulty during the previously described round trip. The rider does not require oxygen nor require medical attention in route. The rider may be transported in a sitting position in a private auto or agency van. Related to this transport, I hereby waive all claims that I may ever have against __(insert name of sponsoring organization)__, its successors and assigns, and its officers, directors, employees and agents (e.g., volunteers), and their heirs, executors, and administrators.
Signed: _________________________________ Date: ________________
3. Volunteer Driver: (Please indicate appropriate responses and sign)
I have read the particular circumstances of this transport and will/will not drive the person named above with/without another person to accept the responsibility of care in route. The undersigned waives all claims arising out of the transport whether caused by negligence, breach of contract or otherwise, and whether for bodily injury, property damage or loss or otherwise, that I may ever have against __(insert name of sponsoring organization)__, its successors and assigns, and its officers, directors, employees and agents and their heirs, executors, and administrators.
Signed: _________________________________ Date: ________________
Wheelchair and Rider Securement Procedures and Checklists
Wheelchair and Rider Securement Procedures* and Checklists (Examples)
*What follows is general information and guidance for wheelchair and rider securement. Programs should ensure that current policies and procedures agree with manufacturer’s guidelines for the securement systems currently in use. For more information about where to find training for volunteer drivers, see Section 4 – Establishing and Managing a Volunteer Driver Pool.
General information about securing wheelchairs.
- Proper securement of the wheelchair and the rider are two of the most important duties a volunteer van driver has when transporting a person who uses a wheelchair or scooter.
- All ADA-compliant buses and vans are required to have a two-part securement system, one to secure the wheelchair, and a seat belt and shoulder harness for the wheelchair user. (Department of Transportation’s Americans with Disabilities Act (ADA) Accessibility Specifications for Transportation Vehicles Section 38.23(d).)
- Wheelchairs meeting the standard set by the American National Standards Institute (ANSI)/Rehabilitation Engineering & Assistive Technology Society of North America (RESNA), ANSI/RESNA standard WC-19 have standardized securement attachment points. For more information on this standard and its applicability to transit and wheelchair transportation, see University of Michigan Transportation Research Institute’s summary of WC19: Wheelchairs.
- For more information on seat belts, see U.S. DOT Questions and Answers Concerning Wheelchairs and Bus and Rail Service Disability Law Guidance web page.
- Wheelchair must be forward-facing.
- The securement system is designed to be used with the wheelchair facing forward.
- Wheelchair securement positions are inherently safer and wheelchairs and the human body are better capable of surviving a frontal crash when facing forward.
- Sled tests show that side-facing wheelchairs are unstable and often collapse.
- Lap and shoulder belt restraint systems are designed to be most effective in the frontal impact position. Wheelchairs are stronger in frontal loading conditions as opposed to side loading.
Procedures for securing the wheelchair. Checklist
- The wheelchair is forward facing.. □
- Center the wheelchair with the anchorages on the floor. □
- Set the brakes on both sides.. □
- If applicable, turn off the wheelchair power.. □
- At a minimum, the front straps must be the same type and the back straps the
same type.. □ - Do not interchange systems.
Use only one manufacturer’s tie-down system for each wheelchair. □ - The wheelchair is anchored at 4 points using the manufacturer’s instructions. □
- Secure the hooks at the end of the straps to appropriate position on the front
and rear of the wheelchair frame. □ - The ratchets are used in back and the cams are used in front. □
- Tighten the back first. □
- Operating the ratchet straps:
- Before attaching the tie-down to the wheelchair/scooter, ensure that
the ratchet strap moves freely on the ratchet spool by pulling back on
the release. □ - While holding the release back, move the ratchet handle to a fully open position. (the handle should be straight). This will allow the strap to move freely on the ratchet spool for adjustment when securing the wheelchair/scooter. □
- The ratchet lever will move freely when Steps A and B are complete.
The ratchet lever will then tighten the strap securely. □ - The ratchet must be left in the fully closed position to complete
the procedure. □ - To release: pull back on the ratchet lever and open the assembly side. □
- The straps are attached properly:
- They are at as close to a 45 degree angle as possible. □
- The angle is no less than 30 degrees and no more than 60 degrees. □
- They are not attached to the wheels or any detachable portion of the wheelchair. □
- They do not bend around any object. □
- They are away from sharp edges or corners. □
- They don’t crisscross. □
- They are not twisted. □
- There is no forward or reverse movement. □
- Never use the 4-point system (wheelchair securement) without
the 3-point (seatbelt and shoulder harness) lap and shoulder belt. □
General information about securing the rider.
- Always use a 3-point system (seatbelt and shoulder harness) to secure the rider.
- The occupant restraint system is separate from the wheelchair securement.
- The 3-point system secures the rider’s pelvis and torso.
- The occupant restraint system can be attached in several ways.
- To vehicle anchorage points.
- To the wheelchair securement system.
- To the wheelchair itself.
- Follow manufactures guidelines.
Procedures for securing the rider Checklist
- Position the lap belt.
- Over the pelvic bones, not the abdomen. . □
- Inside the armrests, between the side panels and the seat cushion. □
- Adjust the lap belt so it is snug. □
- Position the shoulder belt.
- So that it does not cross the riders face or neck. □
- Never under the rider’s arm where it would cross the rib cage. □
- Adjust the shoulder belt to achieve firm but comfortable tension. □
- Never twist the belts. □
- Belts should always lie flat against the body. □
Updated November 2025

A program of the Federal Transit Administration administered by the Neponset Valley TMA
National RTAP is committed to making this website accessible to persons with disabilities. If you need assistance accessing any content on our website or need alternative formats for our materials, please contact us at info@nationalrtap.org or 781-404-5020.